Introduction
Thyroidectomy (total or subtotal removal of the thyroid gland) is a standard intervention for thyroid cancer, large nodules, or severe Graves' disease. After surgery the patient receives lifelong replacement therapy. Per current ATA 2014 guidelines (PMID 25266247), L-thyroxine (levothyroxine, synthetic T4) is first-line. In the US, more than 95% of post-thyroidectomy patients receive it.
But in clinical practice 10–15% of patients on an adequate dose of L-thyroxine and "normal" TSH continue to report fatigue, weight gain, cognitive impairment, hair loss, and depression. This group is central to understanding when the standard fails: enter NDT (Natural Desiccated Thyroid) — a combination T4+T3 tablet.
This article is a clinical breakdown: what NDT is, who is a candidate, how to start, how to titrate, and what pitfalls remain in 2024 after the first FDA approval of an NDT product (ADTHYZA).
🌀
What NDT Is — Biology and History
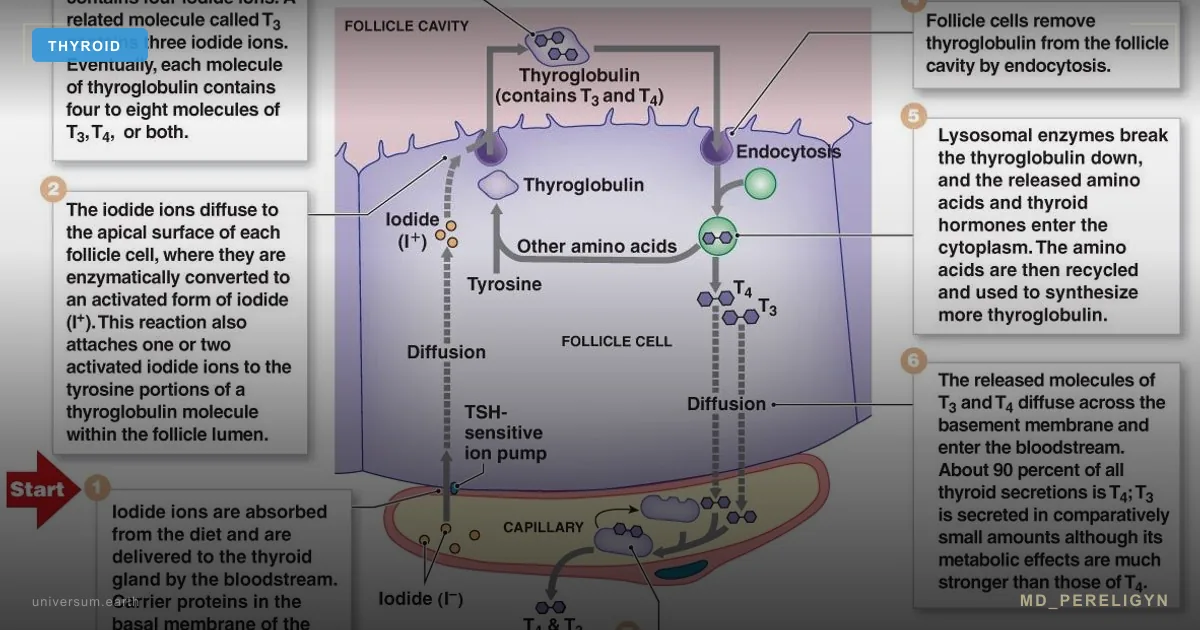
NDT (Natural Desiccated Thyroid; synonyms: desiccated thyroid extract, DTE) is an extract from dried porcine thyroid. It contains both major thyroid hormones in a physiologic ratio: roughly 80% T4 + 20% T3, plus trace amounts of T2, T1, and calcitonin.
Historical timeline:
▸1891 — George Murray described the first injections of sheep thyroid for myxedema ▸1934 — Armour Thyroid launched in the US (Allergan brand) ▸1960s — synthetic L-thyroxine gradually displaced NDT ▸2024 — FDA approved the first DTE product: ADTHYZA (Hikma Pharmaceuticals), now listed in DailyMed
Until 2024 the FDA classified all NDT products as "unapproved drug — other": they were legally sold under a grandfather clause (on the market before 1962) but had not undergone the modern approval pathway. This created the central clinical concern: variable T3 content batch-to-batch, which became the ATA's main argument against routine NDT use.
For background on T4↔T3 conversion biology, see the article on deiodinases and functional hypothyroidism.
🌀
Composition of 1 Grain — Concrete Numbers
Grain is an apothecary unit of mass, historically used in US pharmacy. 1 grain = 60 mg (some labels use 65 mg). This is the NDT dosing unit.
▸1 grain = 60 mg dried extract ▸38 µg T4 (thyroxine) ▸9 µg T3 (triiodothyronine) ▸T4:T3 ratio ≈ 4:1 ▸Clinical equivalence: 1 grain ≈ 100 µg L-T4 (T3 is roughly 3–4× more potent than T4 by biological action)
Standard NDT-to-L-T4 conversion (Jonklaas, ATA 2014, PMID 25266247):
| L-T4 | NDT |
|---|---|
| 75 µg | ¾ grain (45 mg) |
| 100 µg | 1 grain (60 mg) |
| 150 µg | 1½ grain (90 mg) |
| 200 µg | 2 grain (120 mg) |
▸L-T4 100 µg ≈ NDT 1 grain (60 mg) ▸L-T4 75 µg ≈ NDT ¾ grain (45 mg) ▸L-T4 150 µg ≈ NDT 1½ grain (90 mg) ▸L-T4 200 µg ≈ NDT 2 grain (120 mg)
Lab follow-up at 6 weeks after the switch is mandatory — individual response varies.
🌀
US Brands — Current Market
Available DTE products in the US (2024):
▸Armour Thyroid (Allergan) — the oldest brand, on the market since 1934 ▸NP Thyroid (Acella Pharmaceuticals) — generic, similar profile ▸ADTHYZA (Hikma) — the first FDA-approved DTE, approved in 2024, went through modern bioequivalence requirements ▸Niva Thyroid — niche brand ▸Thyroid Tablets USP — multiple generic manufacturers
Discontinued in 2020–2021:
▸Nature-Throid and WP Thyroid (RLC Labs) — company stopped production due to GMP issues
This market narrowing matters clinically: patients stable for years on Nature-Throid were forced in 2021 to switch to Armour or NP Thyroid, and some reported subjective changes (even though formal bioequivalence held).
The 2024 ADTHYZA approval is a landmark: for the first time an NDT product cleared modern FDA stability and active-ingredient requirements. This may gradually shift the ATA position in the next guidelines revision.
🌀
When NDT Is Considered — Clinical Criteria
NDT is not first-line therapy. It is a second step considered when clear criteria are met:
▸Persistent hypothyroid symptoms on normal TSH while on L-T4 — patient on adequate dose for 6+ months, TSH in target range, symptoms persist ▸Low free T3 with adequate free T4 — lab marker of incomplete T4 → T3 conversion (seen in 10–15% of the population) ▸DIO2 polymorphism (Asp92Ala) — genetic variant associated with poor response to L-T4 monotherapy (PMID 19318443 — Panicker et al. 2009) ▸Post-thyroidectomy with low quality of life on T4 monotherapy — especially after total thyroidectomy when no residual gland tissue produces endogenous T3 ▸Hoang RCT 2013 (PMID 23539727) — double-blind crossover trial: 49% of patients preferred DTE over L-T4 monotherapy, especially those with persistent symptoms
A single low free T3 is not enough to switch. The decision requires lab signal + clinical symptom burden + exclusion of other causes (iron, selenium, cortisol, gut). For a systemic breakdown of "normal T4 + hypothyroid symptoms," see the article on rT3 and survival mode.
🌀
Starting Dose and Switching from L-Thyroxine
Starting strategy depends on the patient's baseline:
▸Naive (never on replacement therapy): 30 mg (½ grain) in the morning fasting ▸Switching from L-T4: 1 grain per 100 µg L-T4 (then retitrate by TSH) ▸Older than 65 years or coronary artery disease: 15 mg (¼ grain) start, increase by ¼ grain every 6 weeks — cardiac load from T3 requires caution ▸Pregnancy: NDT is generally not recommended — variable T3 content creates fetal thyrotoxicosis risk in the first trimester. ATA 2017 (PMID 28056690) recommends L-T4 in pregnancy
Example conversion at switch:
▸Patient on 125 µg L-T4 → starting NDT dose 1¼ grain (75 mg) ▸TSH + fT4 + fT3 control at 6 weeks ▸If TSH rises above target — increase by ¼ grain ▸If TSH drops below 0.5 or thyrotoxicosis symptoms appear — decrease
For background on the standard NDT protocol, see the detailed article on hypothyroidism and desiccated thyroid.
🌀
Titration and Target TSH
NDT titration principles mirror those of L-thyroxine, adjusted for the presence of T3:
▸Dose increment: +15–30 mg (¼–½ grain) every 4–6 weeks based on TSH ▸Target TSH: ▸0.5–2.5 mIU/L — benign indications (Hashimoto's thyroiditis, idiopathic hypothyroidism) ▸Risk-stratified for thyroid cancer (per ATA risk categories): low risk 0.5–2.0, intermediate 0.1–0.5, high risk < 0.1 ▸TSH + fT4 + fT3 control at 6 weeks after every dose change ▸Blood draw timing: before the morning NDT dose. Free T3 is falsely elevated if drawn within 4 hours of dosing (T3 peak) ▸Average maintenance dose: 60–120 mg (1–2 grain) in an adult of 60–80 kg
Doses above 120 mg/day are uncommon and require careful clinical-lab justification. Free T3 in the upper third of the reference range is normal on NDT; free T3 above the reference range mandates dose reduction even on a normal TSH.
🌀
Split Dosing — Pharmacokinetics
The key difference between NDT and L-thyroxine is the presence of T3 with its short half-life:
▸T3: half-life ~24 hours — peaks 2–4 hours after dose, falls by evening ▸T4: half-life ~7 days — stable plasma level
This creates a pharmacologic problem: after a single morning dose some patients develop evening T3-deficiency symptoms (fatigue, drowsiness, "afternoon crash"). Solutions:
▸Split dosing: ⅔ dose in the morning + ⅓ dose at midday (e.g., 1–2 PM) — the most common protocol ▸Single-dose schedule — individualized for stable patients ▸Fasting, 30–60 minutes before food, taken with water ▸Avoid coffee, calcium, iron, PPIs in the first hour — same rules as L-thyroxine: these reduce absorption
Evening dosing is contraindicated — T3 disrupts sleep in most patients.
🌀
Monitoring
Lab and instrumental monitoring:
▸TSH + free T4 + free T3 every 6 weeks during dose titration ▸After stabilization — every 6–12 months ▸ECG annually in patients > 50 or with coronary artery disease — T3 increases heart rate and myocardial oxygen demand ▸DEXA (bone densitometry) every 2 years on long-term TSH-suppressive therapy (target TSH < 0.1 for oncologic indications) — accelerated osteoporosis risk ▸Anti-TPO and anti-Tg antibodies at baseline Hashimoto's — once or twice per year to track dynamics
Clinical signs of overdose require immediate dose reduction:
▸Resting heart rate > 100 bpm ▸Hand tremor ▸Sweating, heat intolerance ▸Anxiety, insomnia ▸Weight loss with preserved appetite
Underdose signs:
▸Fatigue, drowsiness ▸Constipation ▸Dry skin, brittle hair ▸Cold intolerance ▸Weight gain ▸Bradycardia < 55 bpm
🌀
Common Pitfalls
Frequent mistakes leading to iatrogenic complications:
▸Self-switching from L-T4 to NDT without an endocrinologist. Especially dangerous in cardiac patients — sudden T3 introduction can trigger arrhythmia or ischemia ▸Dosing "by feel" without TSH control. Subjective sensations do not correlate linearly with lab values; patients push the dose up and arrive thyrotoxic ▸Doses above 120 mg/day without lab justification. High NDT doses in several retrospective series associate with atrial fibrillation and osteoporosis ▸Combining NDT with Cytomel (T3 monotherapy) — double T3 dosing, iatrogenic hyperthyroidism risk ▸Evening dosing — T3 disrupts sleep in most patients ▸Ignoring the free T3 peak at blood draw — fT3 drawn 2–4 hours after the dose is falsely elevated; always draw before the morning dose
🌀
Bottom Line
ATA 2014 (Jonklaas et al., PMID 25266247) and AACE are aligned: L-thyroxine is the first-line standard. NDT is not recommended as primary therapy because of variable T3 content (until 2024 all DTE products were FDA-unapproved) and a lack of long-term randomized trials with hard clinical endpoints (cardiovascular mortality, fractures).
But in select patients with persistent symptoms on adequate L-T4, lab-confirmed incomplete conversion, or genetic markers (DIO2 Asp92Ala), NDT is a justified clinical option. The decision is always shared: patient + endocrinologist + regular lab monitoring. Self-switching without a clinician is categorically not recommended.
The 2024 ADTHYZA approval opens a new chapter: for the first time an NDT product met modern FDA stability and bioequivalence requirements. This may gradually shift the position of professional societies in upcoming guidelines.
🌀
About the Author
I am Dr. Vladimir Pereligyn, endocrinologist and researcher. I specialize in endocrine, metabolic, and autoimmune protocols with a holistic approach and individualized lab diagnostics. Book a consultation — universum.earth/consultation. Daily clinical breakdowns — @md_pereligyn_thyroid.
🌀
Sources
- Jonklaas J et al. *Guidelines for the Treatment of Hypothyroidism* (ATA 2014). [PMID 25266247](https://pubmed.ncbi.nlm.nih.gov/25266247/)
- Hoang TD et al. *Desiccated Thyroid Extract Compared With Levothyroxine in the Treatment of Hypothyroidism: A Randomized, Double-Blind, Crossover Study.* J Clin Endocrinol Metab 2013. [PMID 23539727](https://pubmed.ncbi.nlm.nih.gov/23539727/)
- Panicker V et al. *Common variation in the DIO2 gene predicts baseline psychological well-being and response to combination thyroxine plus triiodothyronine therapy in hypothyroid patients.* J Clin Endocrinol Metab 2009. [PMID 19318443](https://pubmed.ncbi.nlm.nih.gov/19318443/)
- Alexander EK et al. *2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum.* Thyroid 2017. [PMID 28056690](https://pubmed.ncbi.nlm.nih.gov/28056690/)
- Wiersinga WM et al. *2012 ETA Guidelines: The Use of L-T4 + L-T3 in the Treatment of Hypothyroidism.* Eur Thyroid J 2012. [PMID 24782999](https://pubmed.ncbi.nlm.nih.gov/24782999/)
- DailyMed. *ADTHYZA (thyroid tablets, USP) — FDA label.* National Library of Medicine, 2024.
---
*This article is for informational purposes only and does not replace a medical consultation. Before starting any supplements, changing medication, or undergoing diagnostic procedures, discuss the plan with your physician.*
References
- PMID 25266247. PMID 25266247
- PMID 19318443. PMID 19318443
- PMID 23539727. PMID 23539727
- PMID 28056690. PMID 28056690
- PMID 24782999. PMID 24782999