Introduction: the podocyte as the final molecular filter
When people say that “the kidney filters blood,” a membrane sieve comes to mind. This is a useful metaphor, but physiologically it is insufficient. The final molecular filter of the glomerulus is not the basement membrane or the endothelium, but the podocyte: a highly specialized epithelial cell with interdigitating foot processes that form the slit diaphragm.
The total surface area of podocyte foot processes exceeds 1 square meter per kidney. This is the largest epithelial surface structure in the urinary system. Each podocyte covers 2–4 glomerular capillary loops and does not divide in the adult kidney — cell loss is irreversible.
Key point of the md_pereligyn protocol: podocyte loss precedes a rise in serum creatinine by 5–15 years. This is the intervention window in which process reversibility has been demonstrated by peer-reviewed data (Heerspink HJL, NEJM 2020, PMID 32970396[1], DAPA-CKD trial).
In other words: the kidney loses its filter long before clearance falls enough to become visible on standard biochemistry. If caught at the stage of microalbuminuria, CKD can be stopped before dialysis becomes necessary.
🌀
Slit diaphragm architecture
The podocyte is a cell with unique geometry. Primary processes extend from its cell body; secondary foot processes branch from them and interdigitate with the foot processes of neighboring podocytes. Between the foot processes stretches the slit diaphragm — the final molecular filter.
▸Nephrin (NPHS1) — the structural protein of the slit diaphragm; forms a zipper-like lattice. Nephrin mutations cause congenital nephrotic syndrome of the Finnish type. ▸Podocin (NPHS2) — anchors nephrin in the foot process membrane and maintains the signaling integrity of the diaphragm. ▸CD2AP — links nephrin to the actin cytoskeleton of the foot process. ▸Actin cytoskeleton of the foot processes provides mechanical stability under capillary hydrostatic pressure. ▸Negatively charged glycocalyx (heparan sulfates, sialomucins) repels albumin through charge selectivity. ▸Pore size of the slit diaphragm is about 4 nm — retaining molecules larger than albumin (66 kDa).
When any of these components is damaged, the slit diaphragm becomes “leaky” — albumin begins to enter the primary urine. This is podocytopathy.
🌀
Mechanisms of podocyte injury
Loss of podocyte mass is not an “everything broke at once” event, but a cascade with a key fork: foot process effacement → apoptosis or detachment of the podocyte from the basement membrane.
▸Foot process effacement — a reversible stage. Under the influence of hyperglycemia, angiotensin II, or mechanical stress, the actin cytoskeleton reorganizes, and the foot processes lose their structure and fuse into a flat sheet. At this stage, it is reversible. ▸Loss of nephrin and podocin — the slit diaphragm can no longer maintain charge selectivity. Albumin begins to be filtered. Microalbuminuria appears (Reiser J, Annu Rev Med 2013, PMID 23259464[2]). ▸Podocyte apoptosis — induced by angiotensin II through the AT1 receptor, oxidative stress, and AGE products. ▸Podocyte detachment — the cell detaches from the basement membrane and enters the urine. Podocyturia can be measured — it is a direct marker of active cell loss (Wiggins RC, Kidney Int 2007, PMID 17299522[3]). ▸Hypertrophy of remaining podocytes — they compensatorily cover “bare” areas of the basement membrane, but soon become exhausted as well. Hyperfiltration accelerates the process.
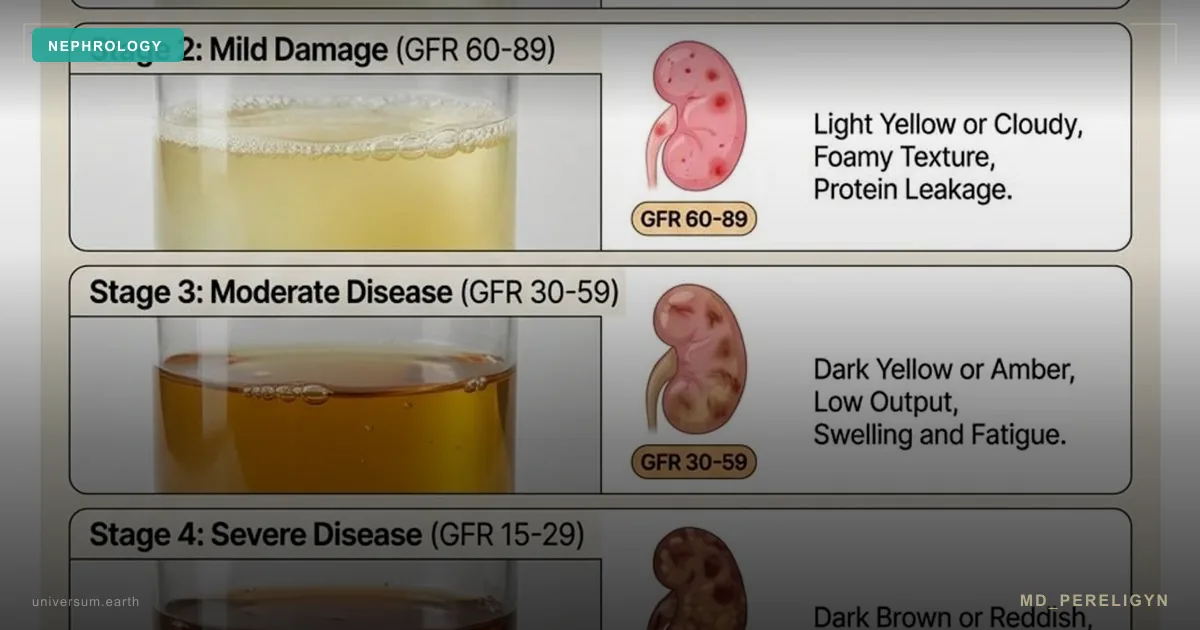
After 5–15 years, the loss of podocyte mass reaches a critical threshold — the remaining cells can no longer compensate, proteinuria increases, glomerular fibrosis progresses, and eGFR begins to fall. Creatinine rises last — when 50–60% of kidney function has already been lost.
🌀
Drivers of podocyte loss
Six factors, each of which independently increases the risk of podocytopathy by 30–60%. In combination, the effect is multiplicative.
•Hyperglycemia — glycation of nephrin and podocin, loss of glycocalyx charge selectivity, formation of AGE products. In patients with type 2 diabetes, podocyte density declines by 0.9% per year even when HbA1c is <7%. •Arterial hypertension — mechanical stretching of foot processes under increased capillary hydrostatic pressure, detachment of podocytes from the basement membrane. BP >140/90 accelerates loss 3–4-fold. •Angiotensin II — induction of podocyte apoptosis through the AT1 receptor, profibrotic signaling (TGF-β). This is a direct target of ACE inhibitors and ARBs. •Oxidative stress — degradation of the actin cytoskeleton, oxidation of BH4 (as in the endothelium), activation of the NLRP3 inflammasome. •Visceral obesity — hyperfiltration driven by adipokines (leptin, resistin), overload of remaining glomeruli. Waist circumference >94 cm in men is associated with a twofold increase in CKD risk. •Long-term NSAID use — reduced prostaglandin synthesis, afferent arteriole constriction, ischemic podocyte injury. Especially dangerous during dehydration.
🌀
Markers of early injury
When a standard clinician says, “creatinine is normal, go home,” early podocytopathy remains unnoticed. What actually reflects podocyte mass status:
▸ACR (albumin/creatinine ratio in morning urine) — the gold standard for early screening. Normal <30 mg/g. Stage A2 (30–300 mg/g) is reversible. A3 (>300 mg/g) requires aggressive renoprotection. ▸Serum cystatin C — more accurate than creatinine in patients with low muscle mass (older adults, women, vegans). Independent of muscle metabolism. ▸eGFR by CKD-EPI 2021 — without race correction; the current standard. Normal >90 mL/min/1.73 m². A decline of >5 mL/min per year indicates progressive CKD. ▸Podocyturia — direct detection of podocytes in urine (nephrin, podocin, synaptopodin). Available in specialized laboratories. ▸Kidney ultrasound with Doppler — renal arterial resistive index (RI). RI >0.7 indicates increased vascular stress. ▸Serum markers: KIM-1 (kidney injury molecule), NGAL, TGF-β — early tubulointerstitial injury. ▸sFlt-1 / VEGF ratio — impaired podocyte-endothelial communication in preeclampsia and nephropathy. ▸Beta-2-microglobulin — a marker of tubular injury.
A detailed discussion of which tests to order first is in the article Microalbuminuria — earliest kidney marker.
🌀
Holistic podocyte support protocol
Principle of the md_pereligyn protocol: treatment is directed not at creatinine, but at the podocyte. Preserving podocyte mass stops CKD progression years before replacement therapy is needed.
### 1. RAAS blockade
▸ACE inhibitor or ARB — lowers intraglomerular pressure by dilating the efferent arteriole. Start with a low dose and titrate to target BP <130/80. Check potassium and creatinine after 1–2 weeks. ▸RAAS inhibitors are indicated when ACR is >30 mg/g even with normal BP — this is renoprotection, not only antihypertensive therapy. ▸Dual RAAS blockade (ACE inhibitor + ARB) is NOT recommended — it increases the risk of hyperkalemia and acute kidney injury.
### 2. SGLT2 inhibitors
▸Dapagliflozin 10 mg or empagliflozin 10–25 mg — renoprotection is proven in CKD with albuminuria and without diabetes (Heerspink HJL, NEJM 2020, PMID 32970396[1], DAPA-CKD). ▸They reduce intraglomerular pressure through tubuloglomerular feedback. ▸They reduce the risk of creatinine doubling and end-stage CKD by 39% (CREDENCE, Perkovic V, NEJM 2019, PMID 30990260[4]). ▸Safe when eGFR is >25 mL/min. Monitor for euglycemic ketoacidosis in patients with type 1 diabetes.
### 3. BP and sodium control
▸Target BP <130/80 — reduces mechanical stress on podocyte foot processes. ▸Sodium restriction <5 g/day — reduces hyperfiltration and potentiates the effect of ACE inhibitors. ▸Dietary potassium (leafy greens, legumes) — only when eGFR is >60 mL/min and serum potassium is normal. If eGFR is reduced, discuss with a physician.
### 4. Anti-inflammatory nutraceuticals
▸Omega-3 (EPA + DHA) 2–3 g/day — reduces systemic inflammation and protects the glycocalyx. Check the omega-3 index every 4–6 months; target >8%. ▸Vitamin D3 2,000–4,000 IU/day — modulates RAAS and podocyte apoptosis; target 25(OH)D level 40–60 ng/mL. ▸Curcumin (liposomal) 500 mg — inhibits TGF-β and the NLRP3 inflammasome. ▸Resveratrol 250–500 mg — activates SIRT1 and preserves podocyte autophagy.
### 5. Antioxidant defense
▸Vitamin C 500–1000 mg — regenerates BH4 and reduces oxidative stress. ▸N-acetylcysteine (NAC) 600–1200 mg — glutathione precursor; protects the podocyte cytoskeleton. ▸CoQ10 100–200 mg — mitochondrial protection for the podocyte (high mitochondrial density). ▸Alpha-lipoic acid 600 mg — especially in diabetic nephropathy.
### 6. Metabolic correction
▸HbA1c <7% — individualized; <8% in older adults. The key is to avoid hypoglycemia. ▸Weight loss when BMI is >30 — even 5–7% reduces albuminuria by 20–30%. ▸Mediterranean / DASH pattern — olive oil, fish, vegetables, nuts, legumes. ▸Protein restriction 0.8 g/kg/day when eGFR is <60 mL/min — reduces hyperfiltration.
### 7. Movement
▸Aerobic activity 30+ minutes/day — improves renal blood flow and lowers sympathetic activity. ▸Moderate intensity — in patients with CKD, intense exercise may provoke transient proteinuria. ▸Strength training 2 times/week — supports muscle mass (important for interpreting creatinine).
🌀
What does NOT work (and why)
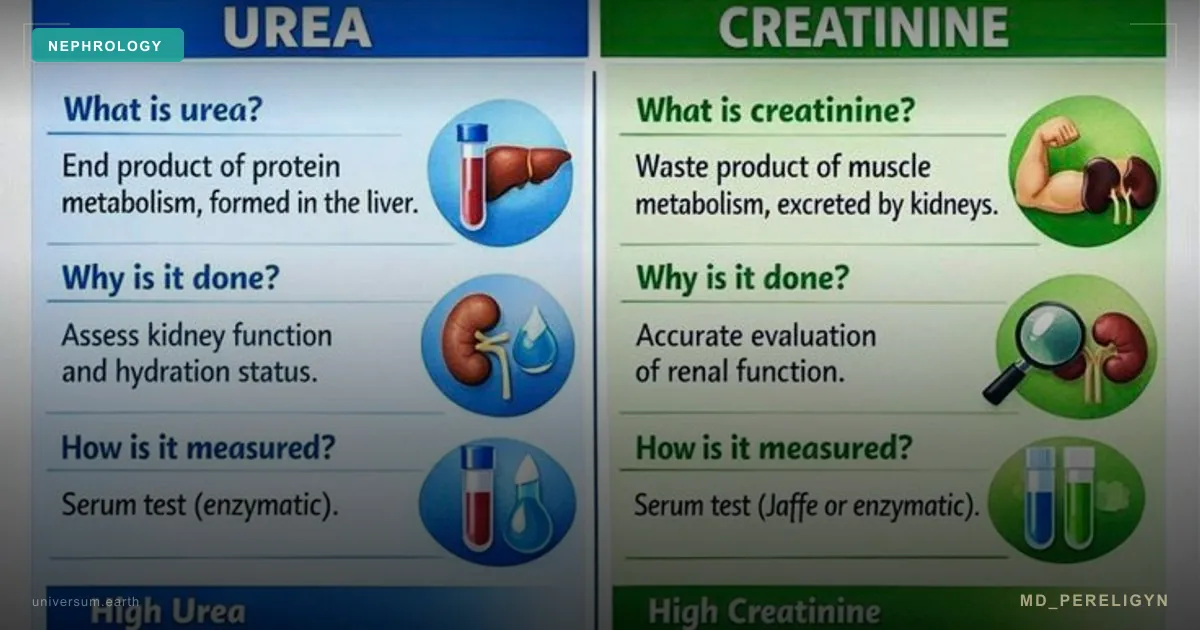
▸Focusing only on creatinine — gives false reassurance. Creatinine remains normal until 50–60% of kidney function has been lost. Use ACR + cystatin C + eGFR together. ▸Long-term NSAID use “for back pain” — prostaglandin blockade, afferent arteriole constriction, podocyte ischemia. Especially dangerous in older adults and during dehydration. ▸Long-term proton pump inhibitors (PPIs) — associated with interstitial nephritis and accelerated eGFR loss (Xie Y, Kidney Int 2017). ▸Dual RAAS blockade (ACE inhibitor + ARB) — increases the risk of hyperkalemia and AKI without additional renoprotection. ▸Ignoring microalbuminuria in a “healthy” patient — this is not a “minor abnormality,” but a signal of podocyte mass loss 5–15 years before creatinine rises. ▸Isolated glycemic control without RAAS blockade — in a person with diabetes, lowering HbA1c to 6.5% does not prevent diabetic nephropathy without RAAS inhibitors and SGLT2 inhibitors.
🌀
When to seek care
▸ACR >30 mg/g in morning urine (even once — repeat after 2–4 weeks for confirmation) ▸eGFR <60 mL/min/1.73 m² or a decline >5 mL/min per year ▸Type 1 or type 2 diabetes of any duration ▸Arterial hypertension lasting >5 years ▸Family history of CKD, dialysis, or kidney transplantation ▸Long-term use of NSAIDs, PPIs, lithium, aminoglycosides ▸Age over 60 years (screening with ACR + cystatin C once per year)
I perform comprehensive nephrology screening (ACR, cystatin C, eGFR by CKD-EPI 2021, ultrasound with Doppler, expanded early-injury panel) and create a personalized renoprotection protocol.
🌀
Conclusion
The podocyte is therapeutic target No. 1 in the nephrology of the future. Not creatinine. Not eGFR in isolation. Not routine urinalysis. The functional state of the final molecular filter of the glomerulus.
Loss of podocyte mass begins 5–15 years before creatinine rises. This is a unique window in which reversibility is proven. A holistic protocol — RAAS blockade, SGLT2 inhibitors, BP and sodium control, omega-3, vitamin D, antioxidants, metabolic correction, and movement — preserves podocyte mass and stops CKD progression.
Treat the podocyte, not its consequences.
🌀
Sources
▸Reiser J, Sever S. Podocyte biology and pathogenesis of kidney disease. *Annu Rev Med* 2013;64:357–366. PMID 23259464 ▸Wiggins RC. The spectrum of podocytopathies. *Kidney Int* 2007;71:1205–1214. PMID 17299522 ▸Heerspink HJL, et al. Dapagliflozin in patients with chronic kidney disease (DAPA-CKD). *N Engl J Med* 2020;383:1436–1446. PMID 32970396 ▸Perkovic V, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy (CREDENCE). *N Engl J Med* 2019;380:2295–2306. PMID 30990260 ▸Nagata M. Podocyte injury and its consequences. *Kidney Int* 2016;89:1221–1230. PMID 27165840 ▸KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. *Kidney Int Suppl* 2024. PMID 37879905
Related articles: Endothelium: foundation of vascular health, Cholesterol without statins.
🌀
FAQ
Can podocytes be restored after many years of diabetes and hypertension? Partially. Podocytes do not divide in the adult kidney, so complete regeneration is impossible. But the remaining cells can exit a “dormant” dysfunctional state, foot processes can recover their structure, and albuminuria can decrease. At stage A2 (30–300 mg/g), reversibility is proven. At stage A3, the goal is stabilization and slowing progression.
Which tests should be done first? Minimum: ACR in morning urine, cystatin C, creatinine with eGFR calculated by CKD-EPI 2021, and routine urinalysis. If possible: kidney ultrasound with Doppler, KIM-1, NGAL. A complete panel and personalized interpretation are provided during consultation.
Are SGLT2 inhibitors safe without diabetes? Yes. DAPA-CKD demonstrated renoprotection in patients with CKD regardless of diabetes status. The main risks are genital mycoses (~5%) and rare euglycemic ketoacidosis. eGFR should be >25 mL/min at initiation.
Should an ACE inhibitor be taken with normal BP if microalbuminuria is present? Yes, when indicated for renoprotection, not antihypertensive therapy. Start with a low dose and titrate. Check potassium and creatinine after 1–2 weeks. The decision is individualized with a physician.
How soon should ACR decrease? After starting an ACE inhibitor + SGLT2 inhibitor + sodium restriction, ACR may decrease by 30–50% within 8–12 weeks. A stable plateau usually occurs by 4–6 months. Check ACR every 3 months until target values are reached, then every 6 months.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 32970396. PMID 32970396
- PMID 23259464. PMID 23259464
- PMID 17299522. PMID 17299522
- PMID 30990260. PMID 30990260
- Nagata M. Podocyte injury and its consequences. Kidney Int 2016;89:1221–1230. PMID 27165840
- KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. Kidney Int Suppl 2024. PMID 37879905