Introduction: a 10-year window
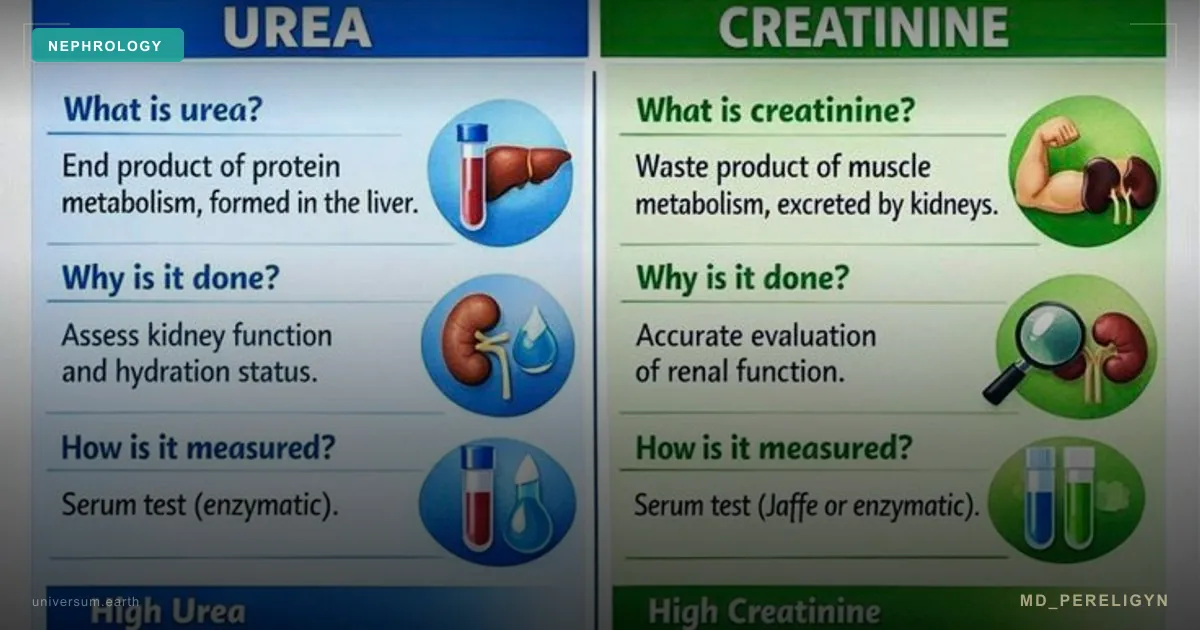
When people say “my tests are good, creatinine is normal,” in most cases it means that kidney damage simply has not yet reached the detection threshold of standard biochemistry. Creatinine is a late marker. It remains within the reference range until 50–60% of kidney function has been lost.
In parallel, there is a test that detects injury 5–15 years before creatinine rises. It is simple, inexpensive, available in any laboratory, and irrationally ignored in routine practice. This is ACR — the albumin/creatinine ratio in a morning urine sample.
Key idea of the md_pereligyn protocol: albumin in urine is the “cry of the podocyte.” It is the most sensitive noninvasive marker of early dysfunction of the glomerular filter. Detecting it 10 years before creatinine rises is the only way to stop CKD before dialysis.
In other words: microalbuminuria is not a “minor deviation that can be ignored.” It is a window for renoprotection in which process reversibility is supported by DAPA-CKD (Heerspink HJL, NEJM 2020, PMID 32970396[1]) and CREDENCE (Perkovic V, NEJM 2019, PMID 30990260[2]).
🌀
What ACR is and why it is more sensitive than creatinine
ACR (Albumin-to-Creatinine Ratio) is the ratio of albumin to creatinine in a single morning urine sample. The creatinine-indexed ratio is used to eliminate the effect of urine concentration (hydration, diuresis).
▸Albumin is a 66 kDa plasma protein that is normally almost completely retained by the podocyte slit diaphragm. <1% of albumin enters the primary urine, and 99% of this filtrate is reabsorbed by the proximal tubules. ▸When podocytes lose slit diaphragm integrity or the glycocalyx degrades, the charge-selective filter can no longer retain albumin. Molecules begin to pass into the primary urine. ▸When tubular reabsorption is overloaded, albumin is excreted in the urine. This is albuminuria. ▸ACR is measured in mg/g (milligrams of albumin per gram of creatinine). An alternative unit is mg/mmol (international system). ▸A morning urine sample is the standard. Not a 24-hour collection. Not a daytime sample. Morning urine is the most concentrated and stable.
Serum creatinine is a marker of function loss that has already occurred. ACR is a marker of an active injury process. They reflect different stages and do not replace each other.
🌀
Normal range and stages of albuminuria (KDIGO 2024)
The modern KDIGO CKD classification divides ACR into three categories — A1, A2, A3. Each has its own prognostic and therapeutic significance.
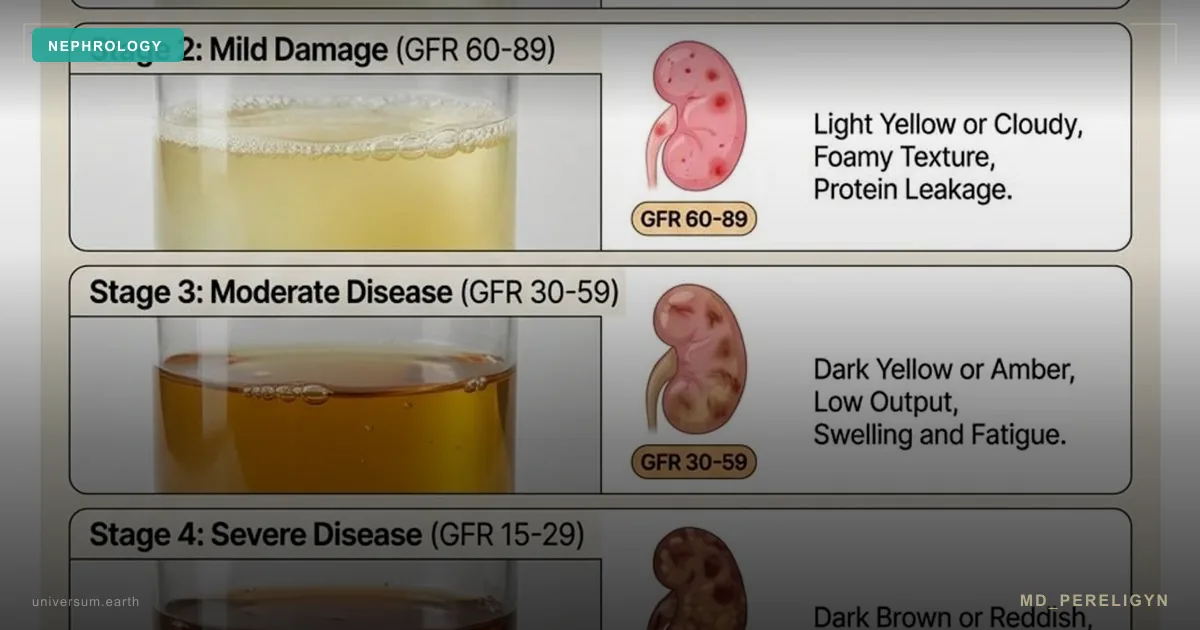
▸A1 — less than 30 mg/g: normal. In patients without risk factors — monitoring once every 3–5 years. In patients with diabetes, hypertension, or family history — once a year. ▸A2 — 30–300 mg/g (microalbuminuria): moderately increased albuminuria. Reversible with early intervention. This is the “10-year window.” Starting an ACE inhibitor/ARB and SGLT2 inhibitor is indicated even with normal blood pressure and without diabetes. ▸A3 — more than 300 mg/g (macroalbuminuria): severely increased. Requires aggressive renoprotection. Prognosis is worse, but progression can be slowed several-fold. ▸A3 + proteinuria >3.5 g/day — nephrotic-range level. Requires kidney biopsy and specialized nephrology care.
Important: one isolated ACR measurement is not sufficient for diagnosis. Albuminuria must be confirmed in two of three consecutive morning samples collected 2–4 weeks apart. Transient albuminuria can occur with fever, exercise, UTI, or dehydration.
🌀
Drivers of albuminuria
Six factors, each of which independently increases the risk of early podocyte injury by 30–60%. In combination, the effect is multiplicative.
•Type 1 and type 2 diabetes mellitus — glycation of nephrin and podocin, loss of glycocalyx charge selectivity. In 30–40% of people with type 2 diabetes, microalbuminuria is already present at diagnosis. •Arterial hypertension — mechanical stretching of foot processes under elevated capillary hydrostatic pressure. BP >140/90 accelerates loss 3–4-fold. •Visceral obesity — hyperfiltration driven by adipokines (leptin, resistin). Waist circumference >94 cm in men is associated with a twofold increase in CKD risk. •Long-term NSAID use — reduced prostaglandins, afferent arteriole constriction, podocyte ischemia. •Autoimmune diseases (SLE, IgA nephropathy, ANCA vasculitis) — immune-complex injury of the basement membrane and podocytes. •Age over 60 years — physiological decline in nephron mass (~1% per year after age 40), reduced glomerular autoregulation.
🌀
Who should have ACR at least once a year
ACR screening is not a narrow subspecialty nephrology test, but part of basic CKD prevention in any adult with risk factors. Indications include:
▸Type 1 and type 2 diabetes mellitus — mandatory from the time of diagnosis, then once a year. ▸Arterial hypertension of any stage — once a year, regardless of BP control. ▸Family history of CKD, dialysis, or kidney transplantation — once a year. ▸Age over 60 years — once a year. ▸Metabolic syndrome, prediabetes (HbA1c 5.7–6.4%) — once a year. ▸Autoimmune diseases — especially SLE, IgA nephropathy, rheumatoid arthritis. ▸Long-term NSAID use (>3 months per year) — every 6 months. ▸Long-term PPI use (omeprazole, esomeprazole >1 year) — once a year. ▸Pregnancy — especially in women with hypertension or diabetes, for early detection of preeclampsia.
The test costs very little. There is no explanation for why it is not done routinely.
🌀
What reduces albuminuria (holistic protocol)
Principle of the md_pereligyn protocol: treatment targets not the ACR number, but preservation of podocyte mass. A 30% reduction in albuminuria is a marker that the protocol is working.
### 1. RAAS blockade
▸ACE inhibitor or ARB — reduces intraglomerular pressure by dilating the efferent arteriole. Start with dose titration to target BP <130/80. ▸Indicated when ACR >30 mg/g even with normal BP — this is renoprotection. ▸Monitor potassium and creatinine 1–2 weeks after initiation. ▸Dual RAAS blockade (ACE inhibitor + ARB) is NOT recommended — it increases the risk of hyperkalemia and AKI.
### 2. SGLT2 inhibitors
▸Dapagliflozin 10 mg or empagliflozin 10–25 mg — ACR reduction by 30–50% within 8–12 weeks. ▸Renoprotection is proven regardless of diabetes status (DAPA-CKD, Heerspink HJL, NEJM 2020, PMID 32970396[1]). ▸Reduce the risk of creatinine doubling and end-stage CKD by 39% (CREDENCE, Perkovic V, NEJM 2019, PMID 30990260[2]). ▸Safe when eGFR >25 mL/min.
### 3. Glycemic and metabolic control
▸HbA1c <7% — individualized, <8% in older adults. The key is avoiding hypoglycemia. ▸Weight loss when BMI >30 — even 5–7% reduces albuminuria by 20–30%. ▸Mediterranean / DASH pattern — olive oil, fish, vegetables, nuts, legumes. ▸Protein restriction 0.8 g/kg/day when eGFR <60 mL/min — reduces hyperfiltration.
### 4. Sodium restriction
▸Less than 5 g of sodium (2 g elemental Na) per day — reduces hyperfiltration and potentiates the ACE inhibitor effect. ▸Without salt restriction, ACE inhibitors/ARBs work 30–40% less effectively. ▸Dietary sodium control is more important than “salt on the table” — the main source is hidden sodium in processed foods.
### 5. Anti-inflammatory nutraceuticals
▸Omega-3 (EPA + DHA) 2–3 g/day — reduces systemic inflammation, protects the glycocalyx. Check the omega-3 index every 4–6 months, target >8%. ▸Vitamin D3 2 000–4 000 IU/day — RAAS modulation, target 25(OH)D 40–60 ng/mL. ▸Curcumin (liposomal) 500 mg — TGF-β inhibition. ▸Vitamin C 500–1000 mg — antioxidant protection of the podocyte. ▸CoQ10 100–200 mg — mitochondrial protection.
### 6. BP control
▸Target BP <130/80 — in patients with ACR >30 mg/g. ▸Home BP monitor + BP diary — mandatory. ▸Morning and evening measurements, 7-day average.
### 7. Movement
▸Aerobic activity 30+ minutes/day — improves renal blood flow, reduces sympathetic activity. ▸Moderate intensity — in patients with CKD, intense exercise may provoke transient proteinuria.
🌀
What does NOT work (and why)
▸“Creatinine is normal — the kidneys are healthy” — this is the most dangerous misconception. Creatinine remains normal until 50–60% of kidney function has been lost. ACR is mandatory in any patient with risk factors. ▸Ignoring microalbuminuria in a “healthy” patient without diabetes — this is a signal of podocyte mass loss 5–15 years before creatinine rises. Renoprotection is indicated. ▸Long-term NSAID use “for back pain” or “for headaches” — prostaglandin blockade, afferent arteriole constriction, podocyte ischemia. Especially dangerous in older adults and during dehydration. ▸Long-term PPIs (omeprazole, esomeprazole >1 year) — associated with interstitial nephritis and accelerated eGFR loss. ▸Dual RAAS blockade (ACE inhibitor + ARB) — increases the risk of hyperkalemia and AKI without additional renoprotection. ▸Isolated glycemic control without RAAS blockade — in a person with diabetes, lowering HbA1c to 6.5% does not prevent diabetic nephropathy without RAAS inhibitors and SGLT2 inhibitors. ▸A “high-protein diet” without eGFR monitoring — a high-protein diet (>1.5 g/kg) increases hyperfiltration and accelerates CKD progression.
🌀
When to seek care
▸ACR >30 mg/g in morning urine (even once — repeat after 2–4 weeks for confirmation) ▸eGFR <60 mL/min/1.73 m² or decline >5 mL/min per year ▸Type 1 or type 2 diabetes mellitus of any duration ▸Arterial hypertension lasting >5 years ▸Family history of CKD, dialysis, or kidney transplantation ▸Long-term use of NSAIDs, PPIs, lithium, aminoglycosides ▸Age over 60 years (ACR + cystatin C screening once a year) ▸Pregnancy with hypertension, diabetes, or history of preeclampsia
I perform comprehensive nephrology screening (ACR, cystatin C, eGFR by CKD-EPI 2021, Doppler ultrasound, expanded early-injury panel) and develop a personalized renoprotection protocol.
🌀
Conclusion
Microalbuminuria is the most underestimated marker in primary medical practice. Not creatinine. Not a routine urinalysis. Not “I feel fine, so everything is fine.” It is a direct signal that podocytes are already losing slit diaphragm integrity.
A 5–15-year window is a unique opportunity to stop CKD before dialysis. A holistic protocol — RAAS blockade, SGLT2 inhibitors, glycemic and BP control, sodium restriction, omega-3, vitamin D, antioxidants — reduces albuminuria by 30–50% within 8–12 weeks and preserves podocyte mass.
ACR is mandatory for any adult with risk factors. At least once a year.
🌀
Sources
▸de Jong PE, Curhan GC. Screening, monitoring, and treatment of albuminuria. *Lancet* 2008;371:2070–2080. PMID 18632391 ▸Heerspink HJL, et al. Dapagliflozin in patients with chronic kidney disease (DAPA-CKD). *N Engl J Med* 2020;383:1436–1446. PMID 32970396 ▸Fox CS, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes. *Lancet Diabetes Endocrinol* 2015;3:514–525. PMID 26028594 ▸KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. *Kidney Int Suppl* 2024. PMID 37879905 ▸Brantsma AH, et al. Urinary albumin excretion as a predictor of the development of hypertension in the general population. *J Am Soc Nephrol* 2008;19:1207–1213. PMID 18094369 ▸Perkovic V, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy (CREDENCE). *N Engl J Med* 2019;380:2295–2306. PMID 30990260
Related articles: Podocyte — gatekeeper of glomerular filtration, Endothelium: foundation of vascular health.
🌀
FAQ
If ACR was 35 mg/g once and then 12 mg/g — is this disease? No. Albuminuria must be confirmed in two of three consecutive morning samples collected 2–4 weeks apart. Transient albuminuria can occur with fever, exercise, UTI, or dehydration. If ACR >30 mg/g in two of three samples, this is already stage A2.
Can ACR be reduced without medications? Partly. Weight loss of 5–7%, sodium restriction <5 g/day, glycemic control, and a Mediterranean dietary pattern reduce albuminuria by 15–25%. But with confirmed stage A2 + diabetes or hypertension, an ACE inhibitor/ARB + SGLT2 inhibitor is the standard of renoprotection.
Are SGLT2 inhibitors safe without diabetes? Yes. DAPA-CKD proved renoprotection in patients with CKD regardless of diabetes status. The main risk is genital mycoses (~5%) and rare euglycemic ketoacidosis. eGFR should be >25 mL/min at initiation.
Which is better — ACR or routine urinalysis? ACR is an order of magnitude more sensitive. Routine urinalysis (dipstick protein) detects proteinuria >300 mg/g, meaning stage A3. Early A2 stages (30–300 mg/g) are completely missed.
How soon should ACR decrease on the protocol? When starting an ACE inhibitor + SGLT2 inhibitor + sodium restriction, ACR decreases by 30–50% within 8–12 weeks. A stable plateau is reached in 4–6 months. Monitor ACR every 3 months until targets are achieved, then every 6 months.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 32970396. PMID 32970396
- PMID 30990260. PMID 30990260
- de Jong PE, Curhan GC. Screening, monitoring, and treatment of albuminuria. Lancet 2008;371:2070–2080. PMID 18632391
- Fox CS, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without diabetes. Lancet Diabetes Endocrinol 2015;3:514–525. PMID 26028594
- KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. Kidney Int Suppl 2024. PMID 37879905
- Brantsma AH, et al. Urinary albumin excretion as a predictor of the development of hypertension in the general population. J Am Soc Nephrol 2008;19:1207–1213. PMID 18094369