Introduction: where CKD really begins
When people discuss chronic kidney disease in a person with diabetes, the image that often comes to mind is an injured podocyte — a cell with interlacing foot processes that maintains the filtration slit. This is true, but it is already a late stage. The real start of injury occurs one level upstream — in the glomerular endothelium (GEnC), the thin lining of the glomerular capillaries.
GEnC is not "ordinary blood vessels." It is a specialized vascular filter with two unique features: 70–100 nm fenestrations (open windows without diaphragms) and a 200–400 nm thick anionic glycocalyx — a gel-like layer of proteoglycans and sialoglycoproteins that maintains a negative charge and prevents albumin from entering the primary urine.
Key point of the md_pereligyn protocol: GEnC injury and glycocalyx shedding precede the onset of microalbuminuria by 5–10 years, and structural podocyte injury by 8–12 years. This is the earliest intervention window in which functional reversibility has been demonstrated in peer-reviewed data (Salmon AHJ, J Am Soc Nephrol 2012, PMID 22773829[1]; Satchell SC, Diabetologia 2008, PMID 18253709[2]).
In other words: CKD in diabetes begins not in the podocyte, but in the endothelium. And it begins long before creatinine or the urine albumin/creatinine ratio moves outside the reference range. If it is detected at this stage, the cascade can be stopped.
🌀
GEnC architecture: a three-layer filter
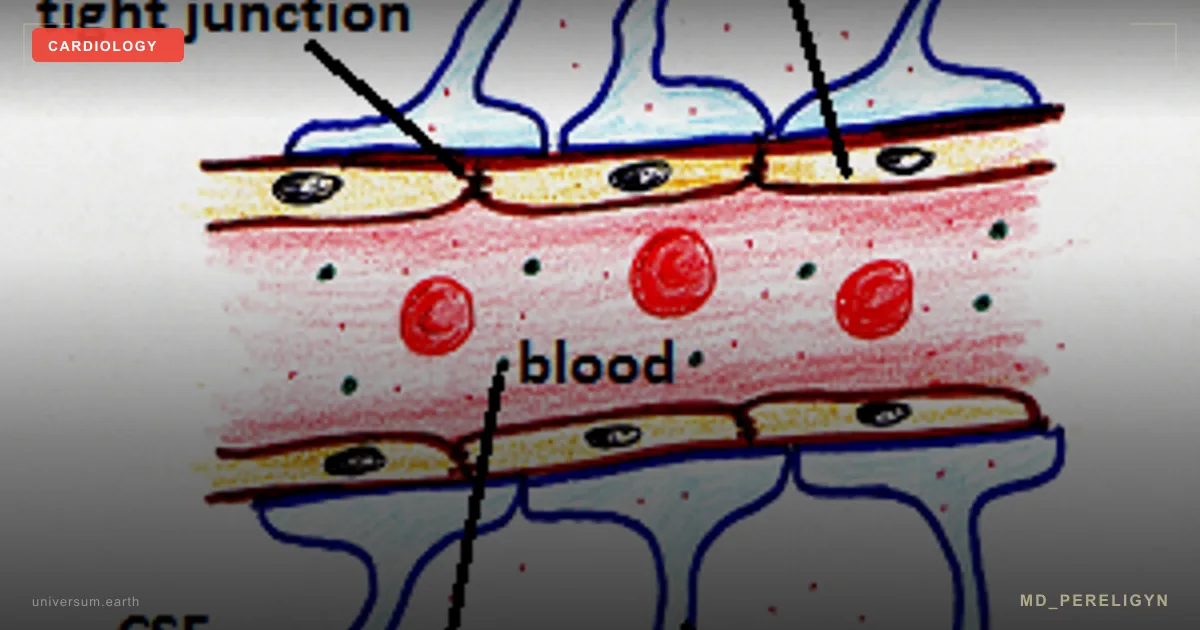
The glomerular filtration barrier is a composite structure with three layers. Each has its own function, and each is necessary:
▸Glomerular endothelium (GEnC) with the glycocalyx — the first and earliest layer. The 70–100 nm fenestrations allow water and electrolytes to pass, while the glycocalyx blocks albumin and other anionic proteins through charge-selectivity. ▸Glomerular basement membrane (GBM) — the middle layer, approximately 300 nm thick, composed of type IV collagen, laminin, nidogen, and heparan sulfate proteoglycans. It provides an additional size and charge barrier. ▸Podocytes with slit diaphragms — the outer layer; nephrin and podocin form the molecular zipper of the approximately 40 nm filtration slit. This is the final line of defense.
All three layers work as a single system. But injury begins from the inside outward: first the endothelium and its glycocalyx, then the GBM, then the podocyte. Standard tests (creatinine, urine albumin) detect only the third stage — when the podocyte is already disrupted and protein begins to leak into the urine.
The total area of GEnC fenestrations is approximately 25% of the entire glomerular surface. This is a large active membrane that filters about 180 liters of plasma per day in an adult. Any disturbance of its function has immediate systemic consequences.
🌀
Mechanisms of GEnC injury
Glomerular endothelial dysfunction is not a single all-at-once failure, but a cascade with two key events: reduced NO bioavailability and glycocalyx shedding.
▸Reduction in eNOS-dependent NO. Under normal conditions, GEnC eNOS (endothelial NO synthase) maintains capillary tone, thromboresistance, and glycocalyx permeability. Hyperglycemia and oxidative stress uncouple eNOS: the enzyme stops producing NO and begins producing superoxide. NO falls, endothelin-1 rises, and vasoconstriction and fibrosis begin. ▸Glycocalyx shedding. Hyperglycemia glycates proteoglycans (syndecan-1, perlecan, versican) and activates heparanase-1 and hyaluronidase-1, which "shave off" the glycocalyx. The anionic charge disappears, and albumin begins to seep through. This is microalbuminuria — but by the time it appears, 30–60% of the glycocalyx has already been lost. ▸Oxidized LDL via the LOX-1 receptor. GEnC expresses LOX-1, which binds oxidized LDL and induces endothelial apoptosis. In a person with diabetes and dyslipidemia, this doubles the rate of injury. ▸Sepsis and SARS-CoV-2. Acute conditions trigger massive glycocalyx shedding through bacterial heparanase or direct viral cytopathic effects. This explains the frequent AKI seen in COVID-19 and sepsis among patients with already subclinical GEnC dysfunction. ▸Chronic inflammation. TNF-α and IL-6 from visceral fat keep the endothelium in an activated state: increased VCAM-1 and ICAM-1 expression, and NF-κB activation.
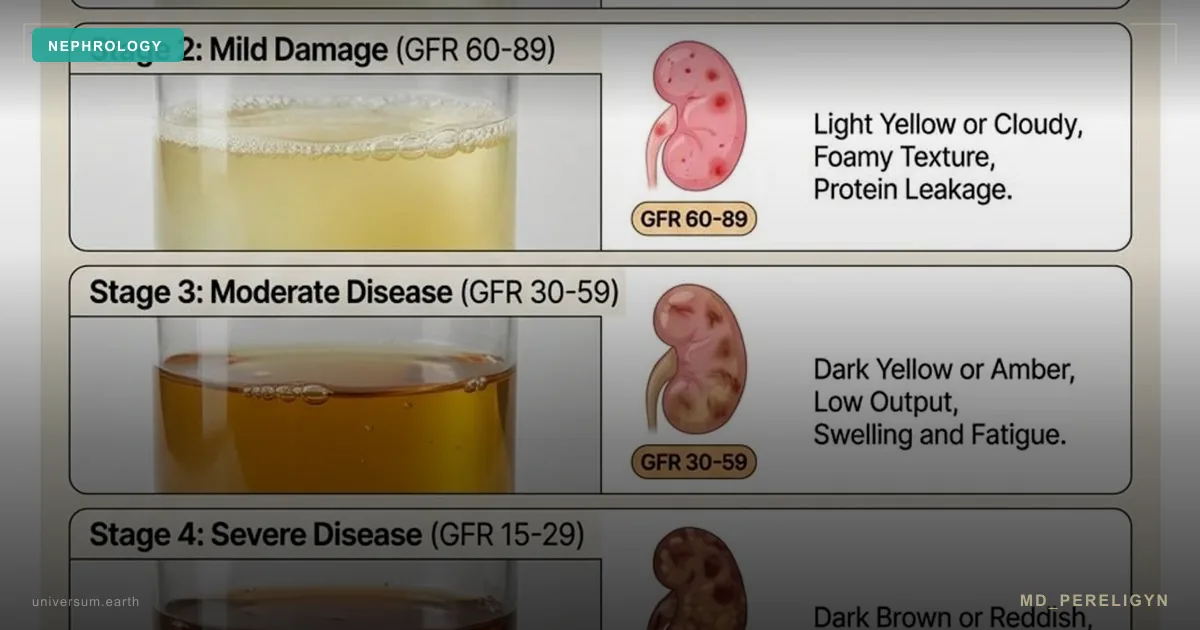
After 5–10 years, glycocalyx shedding reaches the threshold at which microalbuminuria appears (30–300 mg/g in a morning sample). After 10–15 years, macroalbuminuria and declining eGFR develop. Standard nephrology sees only these final stages. The early window remains invisible.
🌀
Drivers of GEnC injury
Seven factors independently accelerate glomerular endothelial injury. In combination, their effect is multiplicative.
•Hyperglycemia and AGE products. Glucose directly glycates glycocalyx proteoglycans and activates RAGE receptors. Even prediabetes with HbA1c 5.7–6.4% is accompanied by subclinical syndecan-1 shedding. •Arterial hypertension. Every 10 mm Hg of systolic pressure above 130 accelerates glycocalyx degradation and increases endothelin-1. Target in the md_pereligyn protocol: BP <130/80 for a person with diabetes, <120/80 for a patient with already detected microalbuminuria. •Dyslipidemia and oxidized LDL. sdLDL and oxLDL bind to LOX-1 on GEnC and induce apoptosis. Target LDL in a patient with diabetes: <70 mg/dL; with microalbuminuria present — <55 mg/dL. •ADMA — asymmetric dimethylarginine. An endogenous eNOS inhibitor; its concentration rises in CKD, diabetes, and hypertension. Each μmol/L increase in ADMA raises renal-vascular risk by 22% (Schnabel R, Eur Heart J 2005, PMID 15843277[3]). •Visceral fat and systemic inflammation. TNF-α, IL-6, and resistin keep GEnC in an activated state. Waist circumference >94 cm (men) / >80 cm (women) is a risk factor independent of BMI. •Smoking. Nicotine reduces eNOS, while carbon monoxide displaces NO from hemoglobin. In smokers with diabetes, the rate of nephropathy progression is 2.5 times higher. •Vitamin D deficiency (<30 ng/mL). Vitamin D regulates eNOS expression and inhibits RAAS activation in the kidney. Deficiency is associated with increased ADMA and faster progression of albuminuria.
🌀
Early biomarkers of GEnC dysfunction
The standard nephrology panel — creatinine, urea, CKD-EPI eGFR, urine albumin/creatinine ratio — detects the kidney at CKD stage 3 and later. Early GEnC injury requires different markers:
▸Serum syndecan-1 — a glycocalyx fragment and marker of active shedding. Normal <50 ng/mL; elevation indicates ongoing GEnC injury. Available in specialized laboratories (Germany, USA). ▸Serum ADMA and SDMA — direct markers of eNOS inhibition and systemic endothelial dysfunction. They rise 5–10 years before eGFR declines. ▸Soluble VCAM-1 (sVCAM-1) — an indicator of endothelial activation, elevated in subclinical vascular inflammation. ▸Cystatin C — a filtration marker independent of muscle mass. It rises earlier than creatinine in lean and elderly patients. ▸Microalbuminuria (ACR 30–300 mg/g) — already a late marker: by the time it appears, 30–60% of the GEnC glycocalyx has been lost. ▸Nailfold capillaroscopy — a surrogate visual marker of microvascular dysfunction associated with GEnC status. ▸Brachial artery FMD <4% — a marker of systemic endothelial dysfunction that also reflects the renal endothelium.
A detailed review of what the standard kidney panel really shows and where its blind spots are can be found in the article Creatinine lies: the limits of the standard kidney panel.
🌀
Holistic protocol for GEnC restoration
The principle of the md_pereligyn protocol: treatment is directed not at creatinine, but at the endothelium and the glycocalyx. Restoring the NO pool and restituting the glycocalyx stops the nephropathy cascade years before dialysis or transplantation becomes necessary.
### 1. NO precursors
▸L-arginine 3–6 g/day — an eNOS substrate; divide into 2–3 doses on an empty stomach. ▸L-citrulline 3 g/day — bypasses first-pass hepatic arginase, more reliably increases plasma arginine and renal NO. ▸Betaine (trimethylglycine) 1500 mg — lowers homocysteine (an independent factor in GEnC injury), a remethylation cofactor.
Caution: if eGFR is already reduced to <45 mL/min/1.73 m², amino acid doses should be adjusted individually with the treating nephrologist.
### 2. Glycocalyx stabilizers
▸Sulodexide 250 LSU twice daily — a heparinoid with demonstrated effects on glycocalyx stabilization in diabetic nephropathy (Khalil RM, Diabetes Res Clin Pract 2018, PMID 29221767[4]). Reduces albuminuria. ▸Glucosamine sulfate 1500 mg — a substrate for synthesis of glycocalyx heparan sulfates. ▸Chondroitin sulfate 1200 mg — support for the proteoglycan component.
### 3. Antioxidant protection
▸Vitamin C 500–1000 mg — regenerates tetrahydrobiopterin (BH4), an eNOS cofactor, and prevents eNOS uncoupling in GEnC. ▸N-acetylcysteine (NAC) 600–1200 mg — a glutathione precursor, shown to reduce oxidative stress in the kidney. ▸Alpha-lipoic acid 600 mg — a dual-soluble antioxidant that regenerates glutathione and vitamin C.
### 4. Polyphenols — BH4 regeneration and endothelial protection
▸Pomegranate (extract) 250–500 mg — punicalagin, with demonstrated effects on FMD and systemic endothelial function (Aviram M, Atherosclerosis 2008, PMID 17726507[5]). ▸Cocoa (flavanols) 500 mg — epicatechin, increases NO bioavailability. ▸Curcumin (liposomal) 500 mg — reduces TNF-α and NF-κB, protecting GEnC from inflammatory injury. ▸Quercetin 500 mg — antioxidant, lowers BP.
### 5. Omega-3
▸EPA+DHA 2–3 g/day — reduces TNF-α, IL-6, and systemic inflammation. ▸Check the omega-3 index every 4–6 months; target >8%. ▸Quality is critical: fish oil must be tested for oxidation (TOTOX <26).
### 6. Vitamin D and magnesium
▸Vitamin D3 to a level of 50–70 ng/mL, with individualized doses of 4,000–6,000 IU/day. Regulates RAAS and eNOS expression in the kidney. ▸Magnesium (glycinate / taurate) 400 mg — an eNOS cofactor, lowers BP, and directly relaxes blood vessels. ▸Vitamin K2 (MK-7) 100–200 mcg — directs calcium into bone and protects against renal artery calcification.
### 7. Glycemic and BP control
▸HbA1c <7% — a mandatory target, ideally <6.5% without hypoglycemia when possible. ▸BP <130/80 for a person with diabetes without albuminuria, <120/80 when microalbuminuria is present. ▸SGLT2 inhibitors (empagliflozin, dapagliflozin) — demonstrated nephroprotective effect (DAPA-CKD, Heerspink HJL, NEJM 2020, PMID 32970396[6]). Reduce albuminuria and slow eGFR decline. ▸ACE inhibitors or ARBs for microalbuminuria — standard first-line therapy.
### 8. Nutrition and movement
▸Mediterranean / DASH pattern — olive oil, fish, vegetables, nuts, legumes. Low in AGE products. ▸Protein restriction to 0.8 g/kg/day when eGFR <60, and to 0.6 g/kg/day when eGFR <30 (under dietitian supervision). ▸Restriction of fructose and fast carbohydrates — fructose directly injures the glycocalyx. ▸Aerobic activity 30+ minutes/day — laminar shear stress activates eNOS in the systemic endothelium, including GEnC.
🌀
What does NOT work (and why)
▸Isolated creatinine monitoring without assessing the glycocalyx and microalbuminuria — misses the early window. Creatinine remains normal until approximately ~50% of filtration is lost. ▸Long-term NSAIDs (ibuprofen, diclofenac) — reduce renal blood flow and accelerate GEnC injury. In patients with diabetes and hypertension, they increase AKI risk by 40–60%. ▸High-protein diets (>1.5 g/kg/day) with reduced eGFR — increase hyperfiltration and accelerate glomerulosclerosis. ▸Excess fructose (juices, agave, syrups) — directly injures the glycocalyx and causes hyperuricemia. ▸Isolated vitamin D without K2 at doses >5,000 IU for prolonged periods — risk of renal artery calcification. ▸Avoiding ACE inhibitors/ARBs out of fear that "they harm the kidneys" — in fact, they provide proven nephroprotection in microalbuminuria. A transient creatinine rise of 20–30% is expected and is not a reason to stop therapy.
🌀
When to seek care
▸Type 1 or type 2 diabetes for more than 5 years ▸Prediabetes with HbA1c 5.7–6.4% and a family history of CKD ▸Arterial hypertension for more than 5 years ▸Microalbuminuria in a single test (requires confirmation and expanded diagnostics) ▸Metabolic syndrome, visceral obesity ▸Family history of CKD, dialysis, kidney transplantation ▸A previous episode of AKI (including COVID-19, sepsis, contrast-induced nephropathy)
I perform full screening for early diabetic nephropathy (syndecan-1, ADMA, cystatin C, ACR, eGFR-CKD-EPI 2021, expanded lipid panel) and prepare a personalized protocol for GEnC restoration and glycocalyx stabilization.
🌀
Conclusion
Chronic kidney disease in a person with diabetes begins not in the podocyte, but in the glomerular endothelium. Glycocalyx shedding and reduction of the NO pool precede microalbuminuria by 5–10 years, and structural podocyte injury by 8–12 years. This is the earliest intervention window in which reversibility has been demonstrated.
The holistic protocol — NO precursors, glycocalyx stabilizers (sulodexide, glucosamine), antioxidants, polyphenols, omega-3, vitamin D + K2, glycemic and BP control, SGLT2 inhibitors — restores GEnC and stops the nephropathy cascade years before creatinine or urine albumin leaves the normal range.
Treatment should target the endothelium, not its complications.
🌀
Sources
▸Salmon AHJ, Satchell SC. Endothelial glycocalyx dysfunction in disease: albuminuria and increased microvascular permeability. *J Am Soc Nephrol* 2012;23:537–545. PMID 22773829 ▸Satchell SC, Tooke JE. What is the mechanism of microalbuminuria in diabetes: a role for the glomerular endothelium? *Diabetologia* 2008;51:714–725. PMID 18253709 ▸Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in patients with chronic kidney disease (DAPA-CKD). *N Engl J Med* 2020;383:1436–1446. PMID 32970396 ▸Khalil RM, Abdo WS, Saad A, Mahmoud EHM. Sulodexide ameliorates renal injury in diabetic kidney disease. *Diabetes Res Clin Pract* 2018;141:235–243. PMID 29221767 ▸Daenen K, Andries A, Mekahli D, et al. Oxidative stress in chronic kidney disease. *Pediatr Nephrol* 2019;34:975–991. PMID 29982878 ▸Schnabel R, Blankenberg S, Lubos E, et al. Asymmetric dimethylarginine and the risk of cardiovascular events. *Eur Heart J* 2005;26:967–971. PMID 15843277 ▸Aviram M, Rosenblat M. Pomegranate juice and atherosclerosis. *Atherosclerosis* 2008;200:39–45. PMID 17726507
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
Can the glomerular endothelial glycocalyx be restored? Yes, partially. Sulodexide 250 LSU twice daily for 6–12 months combined with glycemic and BP control leads to syndecan-1 recovery and an average 25–40% reduction in albuminuria. Full restitution requires 12–24 months of a consistent protocol.
Which tests should be done first if diabetes has been present for 5+ years? Minimum: ACR (albumin/creatinine ratio in a morning sample, not 24-hour urine!), cystatin C, CKD-EPI 2021 eGFR (creatinine + cystatin), HbA1c, expanded lipid panel with sdLDL and Lp(a), 25(OH)D. If possible — syndecan-1, ADMA, homocysteine. The full panel is determined during consultation.
Is it safe to take SGLT2 inhibitors with reduced eGFR? Yes, down to eGFR 20 mL/min/1.73 m² according to the latest KDIGO 2024 recommendations. The key is to monitor dehydration, genital infection risk, and ketoacidosis. A transient creatinine rise of 10–20% during the first 4 weeks is expected and reflects a hemodynamic reduction in hyperfiltration.
How soon should albuminuria decrease after starting the protocol? With the combination of ACE inhibitor/ARB + SGLT2 + sulodexide + BP control, ACR decreases by an average of 30% over 8–12 weeks, with a plateau at 6–9 months. Monitor every 3 months. If there is no effect after 6 months, the protocol should be reassessed, adherence checked, and secondary causes excluded (non-diabetic nephropathy).
Can L-arginine be taken in CKD? Yes, when eGFR >45 mL/min/1.73 m² it is safe at 3–6 g/day under monitoring. With eGFR 30–45, reduce to 2–3 g/day. With eGFR <30, only under individualized nephrologist supervision, because amino acid load increases urea.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 22773829. PMID 22773829
- PMID 18253709. PMID 18253709
- PMID 15843277. PMID 15843277
- PMID 29221767. PMID 29221767
- PMID 17726507. PMID 17726507
- PMID 32970396. PMID 32970396
- Daenen K, Andries A, Mekahli D, et al. Oxidative stress in chronic kidney disease. Pediatr Nephrol 2019;34:975–991. PMID 29982878