Introduction: why “creatinine is normal” does not yet mean “the kidneys are normal”
When a patient brings in a blood test showing creatinine 88 μmol/L in a 65-year-old woman and hears from the physician, “everything is normal, go home,” this is a typical situation in post-Soviet medicine. The problem is that creatinine does not measure kidney function directly.
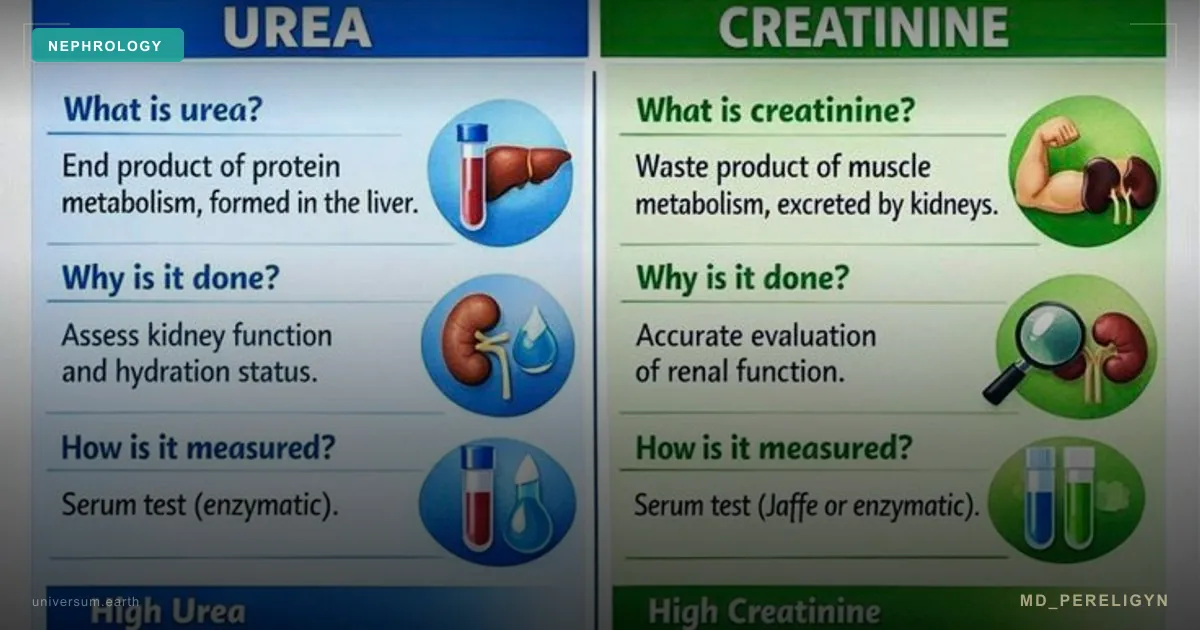
Creatinine is a breakdown product of creatine phosphate in skeletal muscle. Its blood level reflects the balance between two variables: production rate (dependent on muscle mass) and glomerular filtration rate. In a patient with low muscle mass, production is low, and even after losing 40–50% of nephrons, creatinine may remain “normal.”
Key point of the md_pereligyn protocol: creatinine remains within reference values until about 50% of filtration has been lost (Shlipak MG, NEJM 2013, PMID 23984728[1]). This blind window is especially dangerous in thin women, older adults, vegetarians, people recovering after sarcopenia, and patients with cirrhosis or limb paralysis. In these groups, normal creatinine can conceal stage 3A and even stage 3B CKD.
To see the kidney as it really is, creatinine must be supplemented with cystatin C, ACR (albumin/creatinine in a morning urine sample), and the CKD-EPI 2021 equation — the modern standard for calculating eGFR without race correction. This article is a detailed breakdown of what each marker shows, where its blind spots are, and how to assemble a minimal but sufficient panel for early CKD diagnosis.
🌀
What creatinine actually measures
Creatinine monohydrate is the end product of nonenzymatic dehydration of creatine phosphate, the main energy depot in skeletal muscle. Each day, about 1.5–2% of the total creatine pool breaks down in an adult, forming creatinine, which is filtered in the kidney and excreted in urine.
▸Production — proportional to muscle mass. A man with 40 kg of skeletal muscle produces ~20 mg/kg/day of creatinine. A 50 kg woman with low muscle mass produces ~12 mg/kg/day. ▸Glomerular filtration — about 90% of creatinine is excreted through the glomerulus, ~10% through tubular secretion (this “bonus” overestimates calculated eGFR by 10–15% when function is preserved). ▸Tubular reabsorption — practically absent.
The key conclusion follows: creatinine is not a marker of kidney function, but a marker of the “muscle ↔ filtration” balance. If muscle mass is low, low production “compensates” for reduced filtration, and serum creatinine remains normal. This is the main trap.
🌀
Seven creatinine traps
Seven typical clinical situations in which creatinine systematically misleads:
•Low muscle mass (thin women, older adults after 70, patients with sarcopenia or cachexia) — underestimates true CKD. Stage 3A CKD (eGFR 45–59) is possible with “normal” creatinine. •High muscle mass (bodybuilders, professional athletes) — falsely raises creatinine and underestimates calculated eGFR. Actual kidney function may be excellent. •Creatine monohydrate as a supplement (fitness, strength sports) — raises creatinine by 10–20% independently of kidney function. Stop 7 days before testing. •Acute dehydration and shock — prerenal creatinine rise without nephron loss. Resolves after rehydration within 24–48 hours. •Cimetidine and trimethoprim — block tubular creatinine secretion, raising serum levels by 0.1–0.4 mg/dL without a real reduction in GFR. •Liver cirrhosis — reduced hepatic creatine production and loss of muscle mass; creatinine underestimates true renal dysfunction (important in hepatorenal syndrome). •High-protein diet and red meat within 24 hours before testing — raise serum creatinine by 10–15%.
Each of these situations requires confirmation with cystatin C or the combined eGFR-creat-cys equation. Isolated creatinine in these groups is a diagnostic risk, not a diagnostic answer.
🌀
Cystatin C — an alternative without muscle bias
Cystatin C is a low-molecular-weight protein (13 kDa) produced by all nucleated cells in the body at a constant rate. It is freely filtered in the glomerulus, reabsorbed and metabolized in the proximal tubule, and practically does not return to the bloodstream. This makes it an ideal filtration marker.
▸It does not depend on muscle mass, sex, or diet. This is a critical advantage over creatinine in thin women, older adults, vegetarians, and athletes. ▸More accurate than creatinine at BMI <18.5 and >40. In these groups, eGFR-creat error reaches 20–30%; cystatin closes this gap. ▸More accurate in patients >65 years old — the CKD-EPI 2021 cystatin equation shows eGFR closer to the “true” value (measured by inulin or iohexol). ▸Responds earlier to declining kidney function — cystatin C rises after only 30–35% nephron loss, while creatinine rises at 50%. ▸Does not depend on tubular secretion — provides a cleaner estimate of glomerular filtration.
However, cystatin has its own influencing factors: levels increase in hyperthyroidism (accelerated cellular turnover), systemic inflammation (CRP >10 mg/L can overestimate by 10–15%), smoking, and high-dose glucocorticoids. These factors must be considered in interpretation.
Cost: cystatin C in commercial laboratories costs 3–5 times more than creatinine, but its information value in vulnerable groups is many times higher. In the md_pereligyn protocol, cystatin is indicated for all patients over 65 years, all thin women, all athletes, and all cases where a decision about nephrotoxic therapy is being made.
🌀
eGFR CKD-EPI 2021 — the modern calculation standard
The CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation was updated in 2021 and finally removed race correction — the “×1.159 for African Americans” adjustment used since 2009 was recognized as scientifically unsound and eliminated by NKF and ASN decisions.
▸CKD-EPI 2021 creatinine — the basic equation based on serum creatinine, age, and sex. The standard for screening patients with typical muscle mass. ▸CKD-EPI 2021 cystatin C — an equation based on cystatin without creatinine. Use in athletes, cachectic patients, and those with a history of creatine monohydrate use. ▸CKD-EPI 2021 creatinine-cystatin combined — the gold standard for vulnerable groups: older adults, thin patients, suspected stage 3A CKD with “normal” creatinine, and decisions on dosing nephrotoxic drugs. Accuracy approaches measured GFR.
The CKD-EPI 2021 calculator is available online on the NKF website. Any modern laboratory report with creatinine and/or cystatin measurement should include eGFR calculated by CKD-EPI 2021, not the old MDRD or Cockcroft-Gault equations. If your report lists eGFR by MDRD, ask for recalculation.
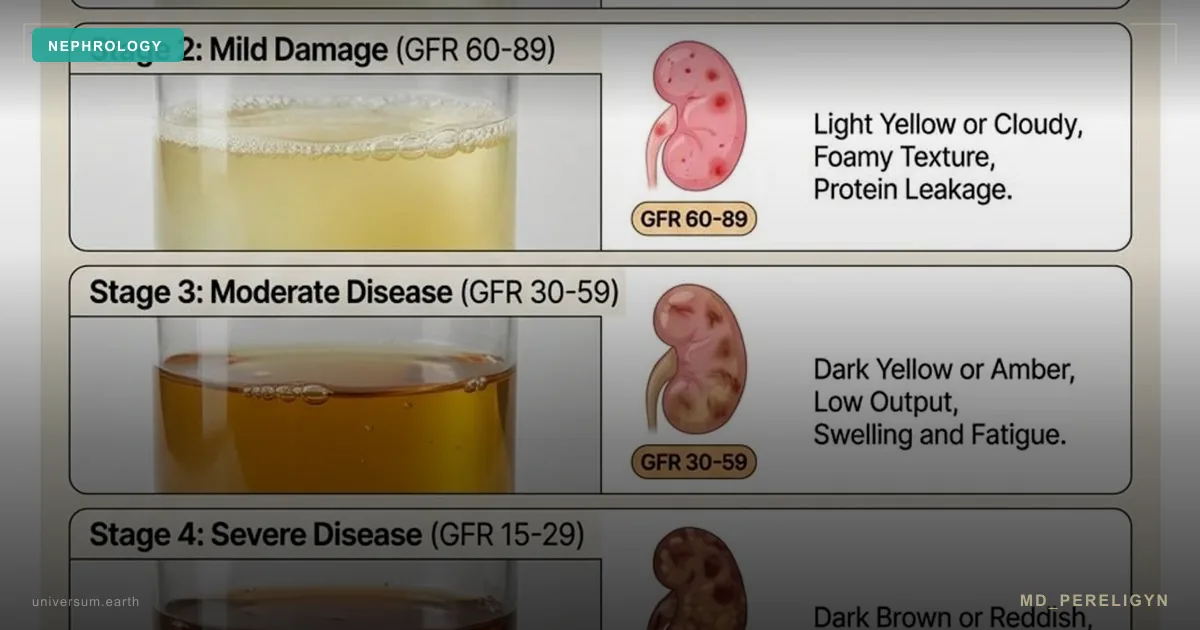
CKD staging by KDIGO (Levey AS, J Am Soc Nephrol 2020, PMID 32646836[2]): ▸G1: eGFR ≥90 (normal or high) + albuminuria ▸G2: eGFR 60–89 (mildly decreased) + albuminuria ▸G3a: eGFR 45–59 (mildly to moderately decreased) ▸G3b: eGFR 30–44 (moderately to severely decreased) ▸G4: eGFR 15–29 (severely decreased) ▸G5: eGFR <15 (kidney failure, dialysis, or transplant)
A decrease in eGFR below 60 mL/min/1.73 m², confirmed over three months, is a diagnostic criterion for CKD. A single value is a reason to repeat testing, not to make a diagnosis.
🌀
ACR — urine albumin/creatinine, the second mandatory marker
eGFR describes filtration function. ACR (albumin-to-creatinine ratio in a morning urine sample) describes barrier permeability — the integrity of the glomerular endothelium and podocyte. These are two independent vectors of CKD staging, and both are mandatory.
▸A1: ACR <30 mg/g — normal. ▸A2: ACR 30–300 mg/g — microalbuminuria. A marker of early diabetic or hypertensive nephropathy. Requires confirmation (at least 2 of 3 tests over 3–6 months). ▸A3: ACR >300 mg/g — macroalbuminuria. Late-stage injury, mandatory ACE inhibitor/ARB therapy.
Important nuances: ▸Morning sample, not 24-hour urine. A 24-hour collection is outdated and inconvenient; a morning sample is sufficient for screening. ▸Ratio to urine creatinine automatically normalizes for urine concentration (diuresis), so absolute albumin content in a random sample is not informative without creatinine. ▸Transient albuminuria can occur after fever, intense physical exertion, dehydration, or urinary tract infection. Confirm after 2–4 weeks. ▸Standard “urine albumin, urinalysis” detects only macroalbuminuria (>300 mg/g) and completely misses microalbuminuria. Order ACR specifically.
🌀
When creatinine must be duplicated with cystatin
Six clinical groups in which isolated creatinine is a diagnostic error and mandatory cystatin C supplementation with calculation by the combined equation is required:
▸BMI <18.5 or >40 — extremes of muscle mass. ▸Age over 65 years — sarcopenia is almost universal. ▸Chronic inflammatory diseases (RA, IBD, systemic lupus erythematosus) — muscle catabolism. ▸Liver cirrhosis, limb paralysis, prolonged immobilization — sharp loss of muscle mass. ▸Professional athletes and strength athletes, creatine monohydrate use — false creatinine elevation. ▸Decision to prescribe nephrotoxic drugs — amphotericin, aminoglycosides, some NSAIDs, contrast agents, lithium salts, cisplatin. Here, underestimating eGFR by 10–15% means overdosing and AKI risk.
In these groups, the minimal package is: creatinine + cystatin C + combined eGFR + ACR from a morning urine sample. Cost in a commercial laboratory (Citilab, Gemotest, Invitro) is about 1,500–2,500 rubles or 25–40 euros.
🌀
What does NOT work (and why)
▸Isolated creatinine in older adults and thin women — misses stage 3A CKD in up to 50% of cases. ▸eGFR by MDRD or Cockcroft-Gault — outdated equations, 10–15% less accurate than CKD-EPI 2021. ▸Race correction for creatinine “×1.159 for African Americans” — officially eliminated in 2021; it must no longer be used. ▸Isolated “urine albumin, urinalysis” — detects only macroalbuminuria and misses early injury. Order ACR specifically. ▸24-hour urine collection for protein and creatinine — outdated, inconvenient, inaccurate because of collection errors. Morning ACR is more informative. ▸eGFR calculation without naming the equation — ask the laboratory which equation is used. If MDRD, request recalculation by CKD-EPI 2021. ▸A single test to diagnose CKD — confirmation over 3 months is required.
🌀
When to seek care
▸Age over 65 years with any history of hypertension or diabetes ▸Thin body habitus (BMI <20) in women with diabetes or hypertension ▸Athletes with suspected CKD based on “high” creatinine ▸Patients taking or planning a course of nephrotoxic drugs ▸Any microalbuminuria in one test (requires confirmation and expanded diagnostics) ▸Family history of CKD, dialysis, kidney transplant ▸Previous episode of AKI (including COVID-19, sepsis, contrast nephropathy) ▸Patients with liver cirrhosis, CHF, prolonged immobilization
I perform comprehensive kidney function screening with calculation by the combined CKD-EPI 2021 equation (creatinine + cystatin C), morning-sample ACR, an expanded nephrology panel (urea, uric acid, electrolytes, phosphorus, PTH when eGFR is reduced), and prepare a personalized monitoring and nephroprotection plan.
🌀
Conclusion
Creatinine is not a marker of kidney function, but a balance between the patient’s muscle mass and the filtration capacity of the glomerulus. In thin patients, older adults, women, vegetarians, and convalescents, isolated creatinine systematically underestimates true CKD and may remain normal after losing 40–50% of nephrons.
The modern standard of early diagnosis is a triad: cystatin C (closes the muscle-bias gap), eGFR by the combined CKD-EPI 2021 equation (the gold standard for accuracy), and ACR in a morning urine sample (describes glomerular barrier permeability). Each marker closes the blind spot of another.
One marker does not describe the kidney. To catch CKD at stage 3A, when reversibility is still possible, a complete panel is needed — not “creatinine is normal, go home.”
🌀
Sources
▸Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race (CKD-EPI 2021). *N Engl J Med* 2021;385:1737–1749. PMID 34554658 ▸Shlipak MG, Matsushita K, Ärnlöv J, et al. Cystatin C versus creatinine in determining risk based on kidney function. *N Engl J Med* 2013;369:932–943. PMID 23984728 ▸KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. *Kidney Int Suppl* 2024;105:S117–S314. PMID 37879905 ▸Levey AS, Coresh J, Tighiouart H, Greene T, Inker LA. Measured and estimated glomerular filtration rate: current status and future directions. *J Am Soc Nephrol* 2020;31:478–490. PMID 32646836 ▸Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function—measured and estimated glomerular filtration rate. *Am J Kidney Dis* 2008;52:5–18. PMID 18794960 ▸Salmon AHJ, Satchell SC. Endothelial glycocalyx dysfunction in disease: albuminuria and increased microvascular permeability. *J Am Soc Nephrol* 2012;23:537–545. PMID 22773829
Related articles: Glomerular endothelium: the kidney’s vascular filter and glycocalyx, Endothelium: the foundation of vascular health.
🌀
FAQ
My creatinine is 75 μmol/L, and the doctor said “everything is normal” — do I need cystatin C? If you are a woman over 60, have a thin body habitus, or BMI <20 — yes, absolutely. In these groups, creatinine systematically underestimates true CKD by 1–2 stages. Minimal panel: cystatin C + morning-sample ACR + eGFR-creat-cys calculation by CKD-EPI 2021.
I take creatine monohydrate for training — how does this affect my tests? Creatine raises serum creatinine by 10–20% independently of kidney function. Stop it 7 days before testing (full washout). If urgent testing is needed, order cystatin C, which is not affected by creatine intake.
What does ACR 45 mg/g mean? Is this already CKD? This is microalbuminuria (category A2). One test is not a diagnosis; confirmation is required in at least 2 of 3 tests over 3–6 months (after excluding transient causes: fever, intense exercise, urinary tract infection). If confirmed, it is a marker of early diabetic or hypertensive nephropathy and an indication for ACE inhibitor/ARB + SGLT2.
How is eGFR by CKD-EPI 2021 different from MDRD? CKD-EPI 2021 is more accurate in the 60–90 mL/min/1.73 m² range (early decline in function), does not use race correction, and has creatinine-based, cystatin-based, and combined variants. MDRD underestimates eGFR when function is preserved and is less accurate in older adults. The modern standard is CKD-EPI 2021.
Do I need a 24-hour urine collection for protein? No, for screening and most clinical tasks, ACR in a morning urine sample is sufficient. A 24-hour collection remains only for specific cases — nephrotic syndrome with severe proteinuria, or assessment of protein losses before nutritional correction. For CKD diagnosis and monitoring, morning ACR is used.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 23984728. PMID 23984728
- PMID 32646836. PMID 32646836
- Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race (CKD-EPI 2021). N Engl J Med 2021;385:1737–1749. PMID 34554658
- KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of CKD. Kidney Int Suppl 2024;105:S117–S314. PMID 37879905
- Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function—measured and estimated glomerular filtration rate. Am J Kidney Dis 2008;52:5–18. PMID 18794960
- Salmon AHJ, Satchell SC. Endothelial glycocalyx dysfunction in disease: albuminuria and increased microvascular permeability. J Am Soc Nephrol 2012;23:537–545. PMID 22773829