Introduction: the De Ritis index as the liver's biochemical fingerprint
In 1957, the Italian pathologist Fernando De Ritis published a paper describing the ratio of two enzymes — aspartate aminotransferase (AST) and alanine aminotransferase (ALT) — as a diagnostic pattern in hepatitis of different etiologies (Botros M, Clin Biochem Rev 2013, PMID 24353357[1]). More than sixty years later, the work has stood the test of time: the De Ritis index remains one of the fastest and least expensive biochemical tools in hepatology.
The principle is simple: ALT is an almost exclusively cytosolic enzyme and predominantly hepatocellular. AST is present in both the cytosol and mitochondria and is expressed in hepatocytes, myocardium, muscle, kidneys, and erythrocytes. When only the hepatocyte cytosol is affected (steatosis, mild hepatitis), ALT rises predominantly, and the ratio is < 1. When injury is deeper and involves mitochondria (alcohol, severe hepatitis, ischemia), AST is released and the ratio increases.
Key point of the md_pereligyn protocol: isolated analysis of AST or ALT is a “temperature reading.” Their ratio is an etiologic pattern. Combined with GGT, platelets, and noninvasive fibrosis scores (FIB-4, NFS, ELF), the De Ritis index gives the physician 80% of the diagnostic map before ultrasound and elastometry.
This is not a replacement for biopsy or FibroScan. It is a first-line tool that identifies the patients who genuinely need those investigations.
🌀
What AST and ALT measure
Both enzymes catalyze transamination reactions — the exchange of amino groups between amino acids and keto acids. These are central reactions in nitrogen metabolism.
▸ALT (alanine aminotransferase) — catalyzes L-alanine + α-ketoglutarate ↔ pyruvate + L-glutamate. Location: hepatocyte cytosol (~95% of activity is hepatic). Plasma half-life ~47 hours. The most specific marker of hepatocellular injury. ▸AST (aspartate aminotransferase) — catalyzes L-aspartate + α-ketoglutarate ↔ oxaloacetate + L-glutamate. It exists in two isoforms: cytosolic (cAST) and mitochondrial (mAST). Location: liver, myocardium, skeletal muscle, kidneys, erythrocytes. Half-life ~17 hours.
In mild hepatocellular injury, the cell membrane is affected and cytosolic contents are released — mainly ALT and cAST. ALT rises higher because of its greater concentration in hepatocytes and longer half-life. Ratio < 1.
In deep injury (necrosis, alcohol-related mitochondrial toxicity, ischemia, fulminant hepatitis), mitochondria are also damaged and mAST is released. AST rises above ALT, and the ratio inverts.
🌀
De Ritis Index: interpretation by range
Six clinical scenarios depending on the ratio:
▸AST/ALT < 1 — the typical pattern of MASLD (metabolic dysfunction-associated steatotic liver disease), viral hepatitis B and C in the inactive phase, and drug-induced injury. ALT predominates: the injury is cytosolic, hepatocellular, and without mitochondrial destruction. ▸AST/ALT 1.0–1.5 — a transition zone: MASLD progression to MASH, early fibrosis, or drug hepatotoxicity is possible. ▸AST/ALT > 1.5 — high probability of alcohol-related liver injury. Williams AL and colleagues (J Hepatol 1988, PMID 3392213[2]) showed that a ratio > 2 has ~96% specificity for alcoholic hepatitis. ▸AST/ALT > 2 + GGT > 100 — practically pathognomonic for acute alcoholic hepatitis. AST rarely exceeds 300–500 IU/L in purely alcohol-related injury (ALT is often <300). If AST > 500, look for another cause. ▸AST/ALT > 1 in cirrhosis of any etiology — the ratio inverts in cirrhosis regardless of the initial cause. This is explained by reduced availability of vitamin B6 (pyridoxal-5-phosphate), an ALT cofactor, and mitochondrial dysfunction. Ratio > 1 in a patient with thrombocytopenia < 150 × 10⁹/L is a strong predictor of cirrhosis (Kim WR, Hepatology 2008, PMID 18537192[3]). ▸AST/ALT >> 5–10 with normal or moderately elevated absolute values — suggests a muscular rather than hepatic origin (rhabdomyolysis, myopathies, intense physical exercise). Check creatine kinase (CK).
Important: in ischemic hepatitis (“shock liver”), AST rises into the thousands during the first 24 hours and then falls rapidly, while ALT follows with a delay. The ratio in the acute phase may be >2, but this does not mean an alcohol-related cause.
🌀
Drivers of AST and ALT changes
Eight clinically significant factors that affect liver enzymes:
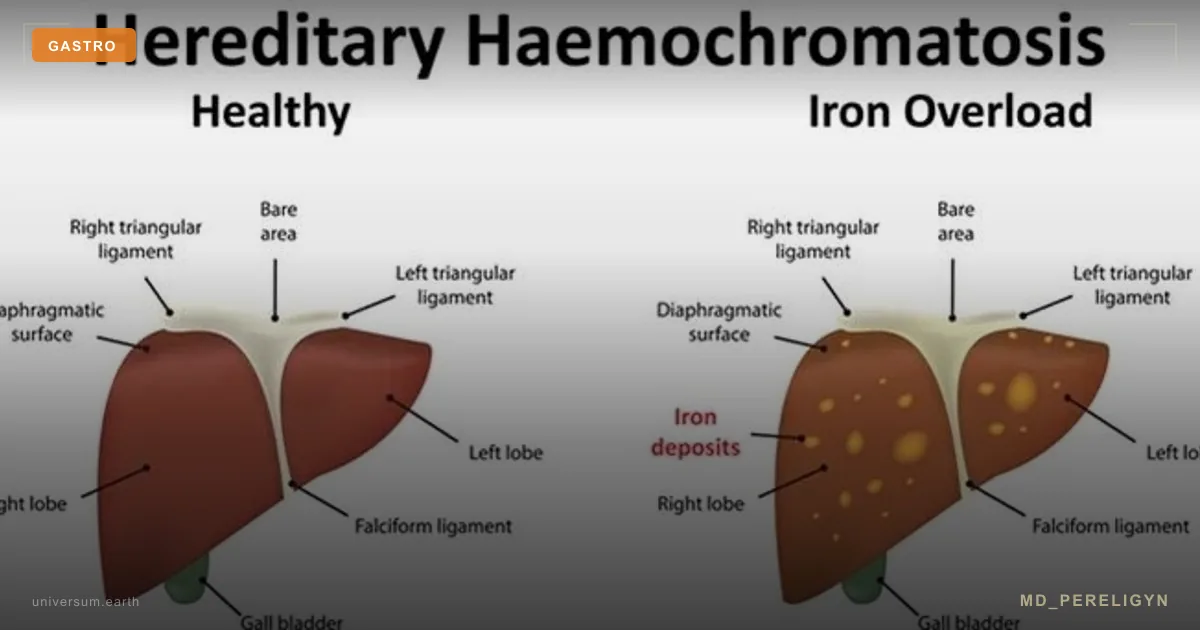
•Alcohol — primarily suppresses B6 synthesis and damages mitochondria. AST > ALT, GGT often > 100 IU/L, mean corpuscular volume (MCV) > 95 fL. •Metabolic syndrome / MASLD — steatosis causes moderate cytosolic injury. ALT > AST. In a patient with BMI > 30 and insulin resistance, an isolated ALT increase of 30–80 IU/L is a typical MASLD pattern. •Drug-induced liver injury (DILI) — statins (rarely, usually ALT < 3×ULN), paracetamol/acetaminophen (>4 g/day), amiodarone, methotrexate, antituberculosis drugs. The pattern depends on the drug. •Viral hepatitis B/C — ALT predominates, ratio < 1 in the active phase. With progression to cirrhosis, the ratio inverts. •Autoimmune hepatitis — a marked ALT response, often > 500 IU/L, elevated IgG, positive ANA / SMA. •Hemochromatosis — moderate ALT and AST elevation (usually <100), TSAT > 45%, ferritin > 300. •Wilson disease — in young patients with ALT/AST elevation + neurological symptoms + Kayser-Fleischer rings. Low ceruloplasmin <20 mg/dL. •Celiac disease — in ~10% of patients with cryptogenic ALT elevation, untreated celiac disease is the cause. Screen with tTG-IgA when the elevation is unexplained.
🌀
Markers: the expanded liver panel
When ALT and AST are elevated, the minimum work-up panel is:
▸GGT — gamma-glutamyl transferase. A sensitive marker of alcohol exposure and cholestasis. > 100 IU/L with a ratio > 1.5 is an alcohol-related pattern. ▸ALP — alkaline phosphatase. Elevated in cholestasis, PBC, and PSC. ▸Albumin and prothrombin time — assessment of hepatic synthetic function. Low albumin and prolonged PT indicate decompensation. ▸Bilirubin (total, direct) — elevated direct bilirubin indicates cholestasis; total with indirect bilirubin suggests hemolysis or Gilbert syndrome. ▸Platelets — < 150 × 10⁹/L + ratio > 1 is a strong predictor of cirrhosis (hypersplenism in portal hypertension). ▸FIB-4 index = (age × AST) / (platelets × √ALT). FIB-4 < 1.3 — low probability of fibrosis; FIB-4 > 2.67 — high probability (F3–F4). Free, fast, and recommended by EASL and AASLD. ▸NFS (NAFLD Fibrosis Score) — includes age, BMI, diabetes, AST/ALT, platelets, and albumin. Specifically validated for MASLD. ▸ELF (Enhanced Liver Fibrosis) — a commercial panel of three fibrogenesis markers (HA, PIIINP, TIMP-1). Accuracy is close to FibroScan and it is available in specialized laboratories. ▸Serologic markers — HBsAg, anti-HCV, ANA, AMA, SMA, ceruloplasmin, ferritin, TSAT, α1-antitrypsin — an etiologic panel. ▸Abdominal ultrasound +, when needed, transient elastometry (FibroScan) — assessment of steatosis and fibrosis stage.
A detailed discussion of ferritin and its interpretation is in the upcoming article Ferritin and the liver.
🌀
Holistic liver recovery protocol
The principle of the md_pereligyn protocol: the laboratory pattern directs treatment toward the etiology, not toward “lowering ALT” as an end in itself. Lowering transaminases without eliminating the cause is cosmetic, not treatment.
### 1. Eliminating the etiology
▸Complete alcohol abstinence when ratio > 1.5 and GGT > 100. Alcoholic hepatitis is reversible with abstinence over 4–12 weeks. ▸Weight loss of 7–10% in MASLD/MASH — the only intervention with convincing evidence for fibrosis regression. It is achieved by combining a caloric deficit, a Mediterranean dietary pattern, and physical activity. ▸Metabolic control — normalization of HbA1c < 6.5%, fasting insulin < 10 mIU/mL, triglycerides < 150 mg/dL. Semaglutide and tirzepatide show MASH regression in RCTs. ▸Withdrawal of hepatotoxic drugs — review all medications with a hepatologist. Many over-the-counter supplements (high-dose green tea, kava, comfrey) are hepatotoxic. ▸Treatment of viral hepatitis C — modern DAA (direct-acting antivirals) achieve SVR > 95% in 8–12 weeks. Hepatitis B — entecavir / tenofovir.
### 2. Antioxidant and mitochondrial support
▸N-acetylcysteine (NAC) 600–1200 mg 2×/day — a glutathione precursor that protects hepatocytes from oxidative stress. Proven in paracetamol/acetaminophen toxicity and alcoholic hepatitis. ▸Silymarin (milk thistle) 140 mg 3×/day — a hepatoprotective agent. Meta-analyses show a moderate reduction in ALT/AST in MASLD and alcoholic hepatitis. ▸Vitamin E 400–800 IU/day — the PIVENS RCT showed histologic improvement in nondiabetic MASH. Do not use in patients with diabetes or coagulopathy without monitoring. ▸Alpha-lipoic acid 600 mg/day — a mitochondrial antioxidant that improves insulin sensitivity. ▸CoQ10 100–200 mg/day — mitochondrial support, especially in patients taking statins.
### 3. Polyphenols and anti-inflammatory agents
▸Curcumin (with piperine) 500 mg 2×/day — reduces ALT in MASLD in RCTs. ▸Green tea (3 cups/day, not high-dose extract) — EGCG is anti-inflammatory. Caution: isolated high-dose extract (>800 mg EGCG) is hepatotoxic. ▸Resveratrol 250 mg/day — a SIRT1 activator, anti-inflammatory. ▸Omega-3 EPA+DHA 2 g/day — reduces liver fat on MRI-PDFF and has anti-inflammatory effects.
### 4. Vitamin D and B-complex
▸Vitamin D3 to a level of 60–80 ng/mL — low vitamin D is associated with fibrosis progression in MASLD. ▸Vitamin B12, folate — deficiency is common in alcohol-related injury and affects methylation and DNA repair. ▸Vitamin B6 (pyridoxine) — an ALT cofactor; deficiency in alcoholism explains the relative decrease in ALT and rise in the ratio. ▸Thiamine (B1) 100 mg/day — mandatory in alcohol-related etiology to prevent Wernicke encephalopathy.
### 5. Nutrition and movement
▸Mediterranean pattern — olive oil, fish, vegetables, legumes, nuts. Proven to reduce steatosis and transaminases in MASLD. ▸Fructose restriction (especially from sugar and corn syrup) — a direct driver of hepatic de novo lipogenesis. ▸Coffee 2–3 cups/day — the only beverage with convincing evidence for liver protection: reduced risk of cirrhosis, HCC, and fibrosis in MASLD. ▸Aerobic exercise 150–300 min/week + resistance training 2–3 times/week — reduces liver fat and insulin resistance.
### 6. Monitoring dynamics
▸Monitor ALT, AST, and GGT every 8–12 weeks during the active treatment phase. ▸Recalculate FIB-4 and NFS every 6 months. ▸FibroScan / ELF — every 12–24 months in patients with F2+. ▸Recovery of the ratio toward < 1 is a sign of moving away from an alcohol-related or cirrhotic pattern.
🌀
What does NOT work (and why)
▸Lowering ALT/AST with “supplements” without addressing the etiology — a cosmetic laboratory effect without stopping fibrogenesis. ▸Isolated vitamin E in patients with diabetes and MASH — data are conflicting, and all-cause mortality may increase at doses >800 IU/day. ▸High-dose green tea extract (>800 mg EGCG) — hepatotoxicity, paradoxical ALT elevation. ▸“Liver cleansing” — detoxes and hepatoprotectors without diagnosis — the etiology is missed (virus, alcohol, hemochromatosis, autoimmune process). ▸Coffee 5+ cups in patients with hypertension and anxiety — even in those whose liver benefits from coffee. Balance with other systems. ▸Long-term hepatotoxic therapy (amiodarone, methotrexate) without monitoring — fibrosis develops without symptoms; screening is needed every 3–6 months.
🌀
When to seek medical care
▸ALT or AST > 1.5×ULN in two consecutive tests ▸AST/ALT > 1.5 — referral for a specific etiology work-up (alcohol, cirrhosis) ▸FIB-4 > 1.3 — elastometry is needed ▸Platelets < 150 × 10⁹/L + elevated enzymes — cirrhosis assessment ▸MASLD factors (BMI > 30, diabetes, dyslipidemia) + any ALT elevation ▸Family history of cirrhosis or hepatocellular carcinoma ▸Persistent ALT elevation > 6 months without an established cause
I perform a full diagnostic work-up — expanded liver biochemistry, serology, FIB-4, NFS, elastometry, and a targeted search for the etiology — and create a personalized recovery protocol.
🌀
Conclusion
The De Ritis index is the most underestimated pattern in the primary diagnosis of liver disease. Ratio < 1 — MASLD pattern. Ratio > 1.5 — look for alcohol. Ratio > 2 + GGT — alcoholic hepatitis. Ratio > 1 + platelets < 150 — cirrhosis.
Each of these scenarios requires different treatment. Treating “elevated enzymes” without understanding the pattern means treating a symptom, not the disease.
Modern hepatology allows a working diagnosis and fibrosis risk assessment in 80% of patients using inexpensive biochemistry and calculated indices (FIB-4, NFS) before referral for FibroScan or biopsy. The key is simply to calculate the ratio and interpret it in context.
🌀
Sources
▸Botros M, Sikaris KA. The De Ritis ratio: the test of time. *Clin Biochem Rev* 2013;34:117–130. PMID 24353357 ▸Williams AL, Hoofnagle JH. Ratio of serum aspartate to alanine aminotransferase in chronic hepatitis. Relationship to cirrhosis. *J Hepatol* 1988;6:181–187. PMID 3392213 ▸Kim WR, Flamm SL, Di Bisceglie AM, Bodenheimer HC; Public Policy Committee of the American Association for the Study of Liver Disease. Serum activity of alanine aminotransferase (ALT) as an indicator of health and disease. *Hepatology* 2008;47:1363–1370. PMID 18537192 ▸Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. *Hepatology* 2006;43:1317–1325. PMID 16729309 ▸Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. *Hepatology* 2007;45:846–854. PMID 17393509
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
If my ALT is 60 IU/L and AST is 30 IU/L, is that bad? This is a typical MASLD pattern (ratio 0.5). By itself it is not critical, but it requires investigation of metabolic status: BMI, waist circumference, HbA1c, fasting insulin, lipids, and liver ultrasound. In confirmed MASLD, the foundation of treatment is 7–10% weight loss and a Mediterranean dietary pattern. Without this, fibrosis progresses in 20–30% over 10 years.
Does AST/ALT 2.5 always mean alcohol? Not always, but it is the first thing to exclude. Alternatives include cirrhosis of any etiology (then platelets are < 150), a muscular etiology (check CK), a history of ischemic hepatitis, or rhabdomyolysis. If alcohol is excluded, elastometry and serology are needed.
Can I drink coffee with elevated transaminases? Yes, and it is even desirable. Coffee is the only beverage proven to reduce the risk of cirrhosis, fibrosis, and HCC in MASLD and chronic hepatitis (meta-analyses by Kennedy O, Aliment Pharmacol Ther 2017). 2–3 cups of ground coffee per day. Without sugar or cream.
Will over-the-counter “hepatoprotectors” help? Only silymarin (milk thistle) and UDCA (ursodeoxycholic acid) for cholestasis have an evidence base. Essential phospholipids, Heptral, and Hepa-Merz have weak data. They do not replace elimination of the etiology. Use only as an adjunct to the main treatment.
How long does it take enzymes to normalize after stopping alcohol? GGT — 2–6 weeks. AST — 2–4 weeks. ALT — 4–8 weeks. If after 12 weeks of complete abstinence the enzymes remain elevated, look for another cause (virus, MASLD, autoimmune process) or early cirrhosis.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 24353357. PMID 24353357
- PMID 3392213. PMID 3392213
- PMID 18537192. PMID 18537192
- Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006;43:1317–1325. PMID 16729309
- Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007;45:846–854. PMID 17393509