Introduction: why "Outlive" is not just another longevity book
Peter Attia is a Stanford-trained physician and longevity researcher, a former oncological surgeon at Johns Hopkins, and the host of *The Drive* podcast. His book "Outlive: The Science and Art of Longevity" (Harmony, 2023) became a #1 New York Times bestseller, but its value lies less in its popularity than in three principles that genuinely change clinical thinking about chronic disease.
I review the book not as a literary critique but as a clinician's notebook — which of Attia's ideas are usable in real preventive practice, which have a solid evidence base, and which warrant caution. The structure of the review follows the logic of the book itself: three core ideas and their clinical implications.
Context matters. Attia practices in the expensive private preventive medicine of California, where a patient can afford ApoB-plus-genetic screening, biannual DEXA scans and a personal trainer. Much of his advice presumes resources that the average patient lacks. But the principles he formulates scale down: they can be applied with a minimal kit — a routine blood panel, an extended lipid panel once a year, regular strength training, and a working stress-management practice. That is why the book matters.
🌀
#first_medicine_must_think_twenty_years_ahead
The central concept of the book is Medicine 3.0. Attia frames it as a shift from a reactive to a proactive model. Modern medicine — which he calls Medicine 2.0 — is built on the twentieth-century infectious-disease paradigm: a disease appears, we treat it. That works for pneumonia, appendicitis, fractures. It loses with atherosclerosis, type 2 diabetes, neurodegeneration and oncology — diseases that take decades to form before clinical manifestation.
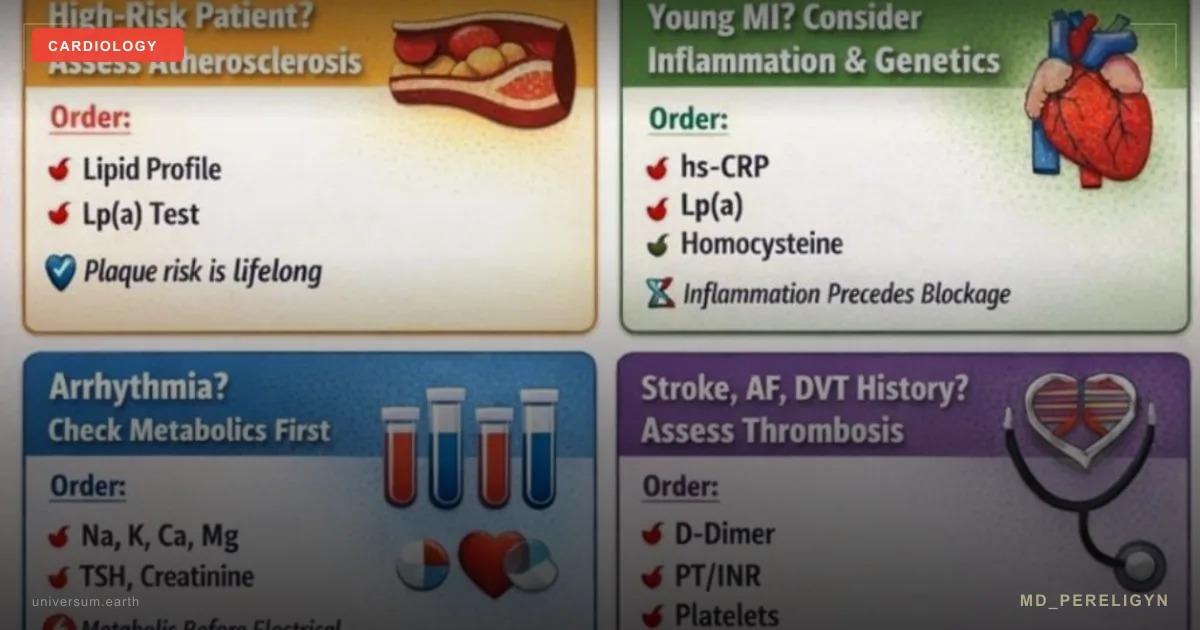
A concrete example from the book is atherosclerosis. Standard practice: measure LDL cholesterol; if it reaches 160 mg/dL discuss a statin. The problem is that by the time LDL has "left the normal range" the plaque has been forming for 10–20 years. Attia proposes an alternative: measure ApoB (the count of atherogenic particles) and Lp(a) (a genetically determined risk factor) at age 30–35. If ApoB exceeds 90 mg/dL or Lp(a) exceeds 50 mg/dL, intervene immediately rather than waiting for a "normative deviation" of LDL.
The evidence base is robust. A meta-analysis of Mendelian randomisation studies (Sniderman AD et al., *Circulation* 2019, PMID 30586722[1]) showed that ApoB is a stronger predictor of cardiovascular events than LDL-C, and that every 10 mg/dL reduction in ApoB correlates with a proportional reduction in risk. Lp(a) is an independent risk factor that statins do not modify and that is genetically determined (Kronenberg F, *Eur Heart J* 2022, PMID 36036785[2]).
Clinical implication: in my practice patients over 30 receive an extended lipid panel — ApoB, Lp(a), small dense LDL — not just total cholesterol and LDL. If ApoB is high while LDL is "normal", that is not reassuring; it is a signal to intervene. If Lp(a) exceeds 75 mg/dL, that is lifelong risk that must be compensated through aggressive ApoB reduction and tight control of other factors (blood pressure, insulin resistance, inflammation).
A typical case in which the difference is visible: a 38-year-old patient, LDL-C 115 mg/dL (formally "borderline high"), no symptoms, family history of paternal myocardial infarction at 52. Standard tactic: "review in a year." Outlive tactic: measure ApoB — 105 mg/dL (markedly elevated), Lp(a) — 88 mg/dL (inherited risk). That is no longer "pre-clinical"; it is the risk level of a 55-year-old with established atherosclerosis. Decision: statin plus lifestyle correction now, not in 15 years when the first plaque appears on a coronary CT.
Attia applies the same principle to diabetes (HbA1c, fasting insulin, HOMA-IR a decade before manifestation), neurodegeneration (early identification of APOE4 carriers and metabolic prevention), and oncology (extended screening for those with a family history).
🌀
#second_the_centenarian_decathlon
The second idea is the most practically valuable. Attia introduces the concept of the Centenarian Decathlon: the goal of longevity is not simply to live to 95 but to retain function at that age. And the function must be specified in concrete, measurable tasks.
The exercise Attia offers every patient: imagine yourself at 90 and write down 10 physical tasks you wish to be able to perform. Examples from his clinic: - Pick up a 12 kg grandchild - Climb three flights of stairs without breathlessness - Get up from the floor without using your hands - Walk 5 km uphill - Open a heavy jar - Lift a 15 kg suitcase onto a shelf - Stand for 30 minutes in a queue without pain - Stand up from a toilet without support - Swim 50 metres - Run 50 metres after a departing bus
Each of these tasks translates into specific physiological reserves: VO2max, muscle mass, grip strength, balance, mobility of hip and shoulder joints. And these reserves must be built decades before they become necessary.
The biology is unsparing. After the age of 30 a person loses 3–5% of muscle mass per decade (sarcopenia), 1% of VO2max per year after 25, and up to 30% of muscle strength between 50 and 70 without targeted training (Cruz-Jentoft AJ et al., *Age Ageing* 2019, PMID 30312372[3]). By 80 an untrained person is balancing at the threshold of functional independence. With training 3–4 times per week over 30–40 years, the same person at 80 lifts a grandchild and runs after a bus.
Clinical implication: training after the age of 50 is not "for the figure" and not "for the heart". It is a specific investment in functional capacity 30 years downstream. In my practice this translates into an individualised plan for every patient over 40: zone 2 cardio for mitochondrial density and metabolic flexibility, resistance training for muscle mass and insulin sensitivity, and balance and stability work as insurance against falls — the single greatest cause of loss of independence at 80.
Zone 2 is itself a key idea of the book. Attia popularised it as low-intensity training (around 60–70% of maximal heart rate, at which one can still speak in full sentences and blood lactate stays below 2 mmol/L). Physiologically, this is the principal regime of mitochondrial adaptation: increased density, fat oxidation, metabolic flexibility. Clinically, it improves insulin sensitivity, lowers triglycerides and raises HDL without overtraining and without cortisol spikes. Minimum dose: three hours per week distributed across 3–4 sessions. For most patients this means brisk uphill walking, cycling at a moderate pace, or long-bout swimming.
Strength training is the second pillar. Attia emphasises two markers: grip strength (a reliable predictor of all-cause mortality — Leong DP et al., *Lancet* 2015, PMID 25908068[4]) and the capacity to carry one's own body weight (a deadlift or a comparable movement within a safe technique). Minimum: two strength sessions per week with a focus on the major compound movements — squat, deadlift, row, press, pull-up. The goal is not records but the preservation of neuromotor patterns across decades.
🌀
#third_the_emotional_foundation
The most personal section of the book. Attia, after years of building protocols for nutrition, training and pharmacology, concedes: none of it delivers longevity if the emotional foundation is broken. He has himself been through clinical depression and intensive psychotherapy, and describes that process with the same scientific precision he brings to biomarkers.
The biological logic of this claim is supported by data. Chronic psychological stress activates the HPA axis, raises cortisol, disrupts the circadian sleep rhythm, raises inflammatory markers (IL-6, TNF-α, CRP), and increases the risk of insulin resistance, visceral adiposity and cardiovascular events (Cohen S et al., *JAMA* 2007, PMID 17925521[5]). Social isolation raises premature mortality by 26–32% — comparable to smoking (Holt-Lunstad J et al., *Perspect Psychol Sci* 2015, PMID 25910392[6]). Unresolved childhood trauma (ACE — Adverse Childhood Experiences) yields lifelong increases in the risk of depression, autoimmune disease, diabetes and oncology (Felitti VJ et al., *Am J Prev Med* 1998, PMID 9635069[7]).
Attia formulates the core point: preventive medicine without work on the emotional foundation becomes self-deception. One can construct an ideal lipid profile and at the same time destroy oneself through chronic loneliness, unresolved conflict, anger or trauma. Biology will count that better than any biomarker.
Clinical implication: in my practice a psychoemotional assessment is a mandatory part of the first consultation, alongside laboratory diagnostics. This does not mean the endocrinologist becomes a psychotherapist. It means I ask about sleep quality, the level of chronic stress, social ties, history of trauma and bereavement. If that domain is impaired, I refer to a specialist in parallel with the metabolic protocol. Treating insulin resistance in a depressed patient is treating the symptom.
Sleep is a separate concrete application of this principle. Attia stresses that 7–9 hours of sleep with intact deep and REM phases is no less important than training or nutrition. Chronic sleep restriction (less than 6 hours) is associated with insulin resistance, accumulation of β-amyloid (an Alzheimer's risk factor), and impaired glucose and testosterone metabolism (Knutson KL et al., *Sleep Med Rev* 2007, PMID 17517353[8]). If a person sleeps 5 hours and trains fasted "for optimisation", they are biologically running in the red zone, masking the problem with a biochemically respectable protocol. Outlive places sleep on a par with the critical interventions.
🌀
#practical_minimum
Re-read with the pragmatic lens of "what can I do starting next week", the book yields a compact list.
Laboratory (annually, after 30): ApoB, Lp(a) (once is enough — a lifetime constant), HbA1c, fasting insulin, HOMA-IR, GGT, ALT/AST, 25(OH)D, ferritin, TSH plus free T3 and free T4, hsCRP. This is the minimum, not the maximum.
Training (weekly): three hours of zone 2 (brisk walking, cycling, swimming) plus two strength sessions (compound movements) plus one short high-intensity session (4×4 intervals or Tabata). Balance and stability work — two short ten-minute blocks per week.
Sleep: 7–9 hours in a 22:30–07:00 window, fixed wake time ±30 minutes (including weekends), last caffeine no later than 14:00, screens off 60 minutes before bed. If sleep is shorter than 7 hours for more than two consecutive nights, recovery takes priority over training.
Psychoemotional: one stable social tie (friend, partner, therapist) with regular contact, the ability to recognise stress triggers, and at least one weekly activity without a productive aim (meditation, a walk without podcasts, a hobby). At markers of depression (PHQ-9 ≥ 10), chronic anxiety or trauma symptoms, seek clinical help — do not assume it will pass.
This is not optimisation. It is the baseline infrastructure that a person builds for their own functional capacity 30 years hence.
🌀
#critique
What is strong in the book: an ApoB-first approach to atherosclerosis, the concept of zone 2 cardio, the reframing of resistance training as functional investment, and an honest section on the psychoemotional dimension.
What requires caution: Attia in places recommends protocols (for example, aggressive ApoB reduction in young patients with PCSK9 inhibitors) on the basis of mechanistic logic that runs ahead of clinical trials on population outcomes. That is not a mistake, but it requires individualised decision-making rather than blind adoption.
What is critically important to understand: the book is written for a healthy person who wants to optimise the trajectory of ageing. It is not a textbook for the treatment of established disease. A patient with an active infarct, decompensated diabetes or oncology requires standard evidence-based therapy first. The Outlive approach is what is done between and after, so that the same does not recur in another ten years.
What Attia omits or underweights: the role of the microbiome and of environmental exposures (heavy metals, endocrine disruptors, air quality) is barely considered. Hormonal status — particularly in women in perimenopause and postmenopause — is discussed superficially. Thyroid function, the hypothalamic-pituitary axis and adrenal regulation are absent. From an endocrinologist's point of view that is a gap: metabolic health without an understanding of hormonal regulation is only half the picture. In my clinical practice the Outlive approach is therefore the skeleton onto which endocrinological assessments and protocols are layered.
🌀
#summary
"Outlive" is not a book about supplements or diets. It is a book about changing the time horizon of clinical thinking. Its three ideas can be summarised in a single sentence: think 20 years before disease becomes obvious; have a concrete functional target you are training for today; and do not ignore the emotional foundation — biology will count it.
🌀
#about_the_reviewer
Dr. Vladimir Pereligyn — endocrinologist. Functional medicine with a focus on preventive strategies: metabolic health, thyroid function, hormonal balance, and individualised risk profiling based on extended laboratory diagnostics. Consultations in person and online: universum.earth/consultation. App Store: Teremok (type 2 diabetes, remission).
🌀
Source
▸ Attia P. *Outlive: The Science and Art of Longevity*. Harmony, New York, 2023. ISBN 978-0593236598. 496 pages.
Further reading on the topics of this review: ▸ Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. *JAMA Cardiol* 2019;4(12):1287-1295. PMID 31642874 ▸ Kronenberg F, Mora S, Stroes ESG, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. *Eur Heart J* 2022;43(39):3925-3946. PMID 36036785 ▸ Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. *Age Ageing* 2019;48(1):16-31. PMID 30312372 ▸ Holt-Lunstad J, Smith TB, Baker M, et al. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. *Perspect Psychol Sci* 2015;10(2):227-237. PMID 25910392 ▸ Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. *Am J Prev Med* 1998;14(4):245-258. PMID 9635069
🌀
*This review reflects the author's clinical interpretation and does not replace consultation with a physician. Before changing therapy, diagnostic protocols or lifestyle, discuss the plan with your treating specialist.*
References
- PMID 30586722. PMID 30586722
- PMID 36036785. PMID 36036785
- PMID 30312372. PMID 30312372
- PMID 25908068. PMID 25908068
- PMID 17925521. PMID 17925521
- PMID 25910392. PMID 25910392
- PMID 9635069. PMID 9635069
- PMID 17517353. PMID 17517353
- Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. JAMA Cardiol 2019;4(12):1287-1295. PMID 31642874