Introduction: “hepatoprotector” as a pharmacological fiction
The term “hepatoprotector” does not exist in American or European guidelines (EASL, AASLD). This category was created by the post-Soviet and Eastern European pharmaceutical market and is sustained there by intensive advertising and by physicians’ habit of prescribing “something for the liver” with any ALT elevation.
Essentiale has been sold since 1953, Heptral (ademetionine) since 1979, Carsil (silymarin) since the 1970s, and Hofitol (artichoke) since the 1950s. The combined market for “hepatoprotectors” in the CIS is estimated at hundreds of millions of dollars per year. Yet by strict evidence-based medicine criteria, most of these drugs have no randomized controlled trials (RCTs) with hard endpoints — biopsy histology, fibrosis, or liver-related mortality.
Key thesis of the md_pereligyn protocol: in MASLD (metabolic dysfunction-associated steatotic liver disease, formerly NAFLD/NASH) — now the most common chronic liver disease worldwide — what works is lifestyle and metabolic change, not a pill. Among supplements, there are a few exceptions with real data. I review them below.
The goal of this article is to separate what has been shown in peer-reviewed RCTs from what is sold through habit and advertising.
🌀
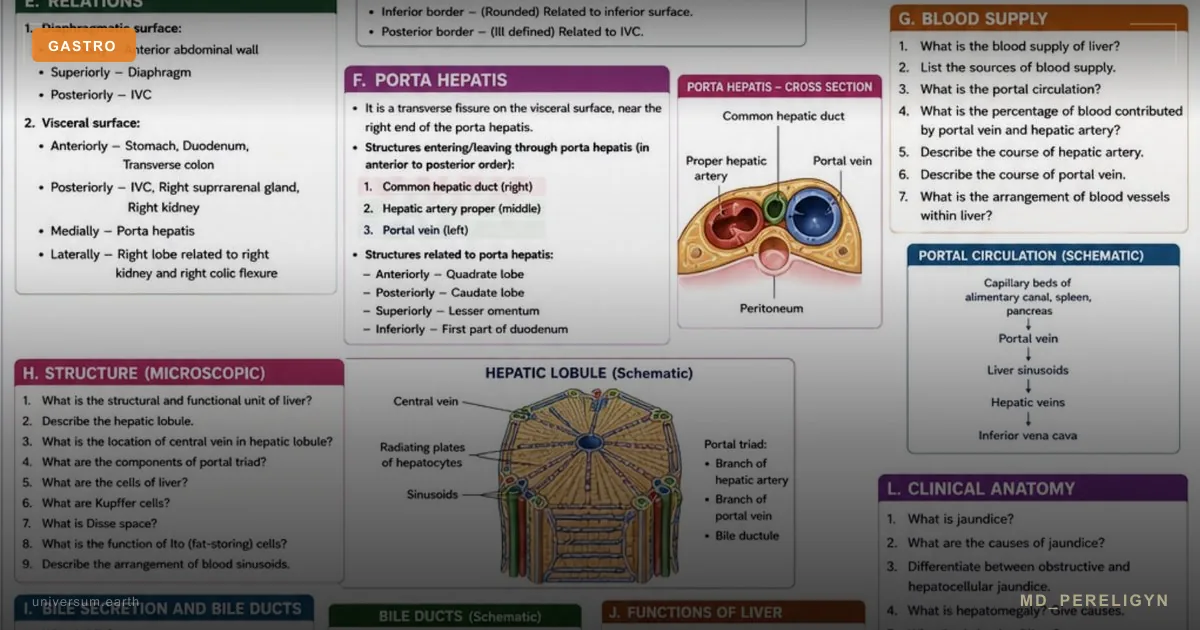
Anatomy of the problem: what MASLD is and why it matters
MASLD (Metabolic dysfunction-Associated Steatotic Liver Disease) is the updated 2023 nomenclature (Rinella ME, Hepatology 2023, PMID 37363821[1]), replacing NAFLD. Global prevalence is about 30% of the adult population, and 55–75% in populations with obesity and type 2 diabetes.
Disease spectrum: ▸Simple steatosis — fatty infiltration without inflammation. ▸MASH (formerly NASH) — steatohepatitis: fat + inflammation + hepatocyte injury (ballooning). ▸Fibrosis F1–F4 — scarring. ▸Cirrhosis and hepatocellular carcinoma (HCC) — endpoints.
The key feature of MASLD: it is the hepatic manifestation of insulin resistance. Visceral fat, hyperglycemia, dyslipidemia, and hepatocyte lipotoxicity share the same pathogenesis. Therefore, treating the liver in MASLD means treating whole-body metabolism.
🌀
What really works (according to RCTs)
A brief list of interventions with solid data:
▸Weight loss of 7–10% from baseline — the only strategy with histologically confirmed regression of MASH and fibrosis (Vilar-Gomez E, Gastroenterology 2015, PMID 25865049[2]). A 5% reduction improves steatosis; 7% improves inflammation; 10% improves fibrosis. ▸Vitamin E 800 IU/day (natural D-α-tocopherol) — in NON-diabetic patients with biopsy-confirmed MASH. The PIVENS trial (Sanyal AJ, NEJM 2010, PMID 20427778[3]) showed histological improvement vs placebo. Included in the AASLD guideline as an option (Chalasani N, Hepatology 2018). ▸Silymarin 420–700 mg/day (standardized milk thistle extract, not Carsil without a specified silibinin dose) — a meta-analysis showed a moderate reduction in ALT/AST across various chronic liver diseases, but the effect on histology and fibrosis is weak or absent (Loguercio C, Drugs 2012, PMID 22994537[4]). It works best in combination with phosphatidylcholine (silyphos). ▸N-acetylcysteine (NAC) 600–1200 mg 2–3 times/day — in acute acetaminophen overdose, it is a life-saving protocol (intravenous). In chronic MASLD, small RCTs show ALT improvement, but the evidence is insufficient for routine recommendation. ▸Coffee 2–4 cups per day — large cohorts show a 30–40% reduction in the risk of cirrhosis and HCC (Kennedy OJ, Aliment Pharmacol Ther 2017, PMID 28166877[5]). The effect is dose-dependent. ▸Semaglutide and pioglitazone — RCTs showed MASH regression (ESSENCE 2024, PIVENS pioglitazone arm). These are prescription drugs for subgroups of patients with type 2 diabetes or obesity.
🌀
What does NOT work (or works only in marketing)
Drugs with billion-scale sales and no convincing evidence base:
•Essentiale (essential phospholipids, EPL) — a 2020 meta-analysis did not confirm hard clinical benefits in MASLD/MASH (Maev IV, World J Gastroenterol 2020). The FDA has not approved the drug. It is included only in local post-Soviet guidelines. RCTs with histological endpoints are absent. •Heptral (ademetionine, SAMe) — the only relatively reliable RCT (Mato JM, J Hepatol 1999, PMID 10579655[6]) in alcoholic cirrhosis showed a reduction in mortality and transplantation — but only in a subgroup and with serious methodological caveats. A 2006 Cochrane review (Rambaldi A) did not confirm clinical benefit in ALD/MASLD. High price, low bioavailability of the oral form. •Carsil (silymarin marker) — contains a low and non-standardized dose of silibinin. It should not be confused with research-grade silymarin at doses of 420 mg (see above). •Hofitol (artichoke extract) — weak data for a choleretic effect, no RCTs with hard endpoints for MASLD/MASH. •Ursodeoxycholic acid (UDCA) in simple MASLD — several RCTs did not show histological improvement (Lindor KD, Hepatology 2004, PMID 15239089[7]). It is indicated for PBC (primary biliary cholangitis) and gallstone disease, but not for MASLD. •“Hepa-Merz” (L-ornithine-L-aspartate) — used in hospital care for hepatic encephalopathy, but not as an outpatient “hepatoprotector.” •“Thioctacid” (alpha-lipoic acid) in MASLD — small studies with conflicting results; not recommended by guidelines.
General pattern: drugs sold as “hepatoprotectors” were developed before the era of mandatory histological endpoints in hepatology RCTs. Their effect on ALT is weak and does not translate into improved histology or prognosis.
🌀
The md_pereligyn holistic protocol
Principle: lifestyle and metabolism first, then a narrow list of supplements with RCT data, and prescription drugs only in individually indicated cases.
### 1. Metabolic foundation (priority No. 1)
▸Weight loss of 7–10% — target rate 0.5–1 kg/week. ▸Mediterranean diet or low-carbohydrate diet (<30% of energy from carbohydrates) — both outperform low-fat diets in their effect on steatosis (Properzi C, Hepatology 2018, PMID 29476613[8]). ▸Fructose restriction (especially from sweetened beverages and HFCS corn syrup) — fructose directly stimulates de novo lipogenesis in hepatocytes. ▸Alcohol reduction to zero in confirmed MASH/fibrosis. In simple steatosis — no more than 1 serving/day for women, 2 for men. ▸Aerobic exercise 150 min/week + resistance training 2–3 times/week — reduces steatosis even without weight loss.
### 2. Methylation and choline
▸Choline 425 mg (women) / 550 mg (men) — dietary reference intake. Choline deficiency in humans causes steatosis within 6 weeks (Zeisel SH, Annu Rev Nutr 2006, PMID 16848706[9]). Sources: eggs (1 egg ≈ 150 mg), liver, fish, soy. ▸Betaine (trimethylglycine) 1500–3000 mg/day — a methyl-group donor that supports phosphatidylcholine synthesis and lowers homocysteine. Especially useful with MTHFR variants. ▸Vitamins B6, B9 (folate, methylfolate), B12 — cofactors of the methylation cycle.
### 3. Antioxidant protection
▸Vitamin E (D-α-tocopherol) 400–800 IU — in NON-diabetic patients with MASH. In patients with diabetes, discuss with a physician; there is a risk of hemorrhagic stroke with long-term high-dose use. ▸N-acetylcysteine (NAC) 600 mg 2 times/day — a glutathione precursor, especially useful with concomitant toxic exposures, acetaminophen, or alcohol. ▸Glutathione (liposomal) 250–500 mg or its precursors (glycine 3 g + cysteine 500 mg).
### 4. Silymarin — if used, use it correctly
▸Silymarin (standardized) 420–700 mg/day, divided into 2–3 doses with food. Its effect on histology is weak, but ALT-AST reduction has been documented in meta-analyses. ▸Silymarin + phosphatidylcholine (silyphos) — better bioavailability. ▸Do not confuse it with cheap “milk thistle” dietary supplements without declared silibinin content.
### 5. Coffee and tea
▸Coffee 2–4 cups/day — a consistent association with lower risk of cirrhosis and HCC. The effect persists for decaffeinated coffee, pointing to the role of coffee polyphenols, not caffeine alone. ▸Green tea (EGCG) — moderate data for steatosis reduction in small RCTs.
### 6. Omega-3
▸EPA+DHA 2–4 g/day — meta-analyses (Parker HM, J Hepatol 2012, PMID 22023985[10]) showed a reduction in liver fat in MASLD. Quality is critical: TOTOX <26.
### 7. Vitamin D
▸Vitamin D3 to a level of 40–60 ng/mL (100–150 nmol/L). Deficiency is associated with MASH progression; correcting deficiency is reasonable, but vitamin D monotherapy does not treat MASLD.
### 8. Sleep and circadian rhythms
▸Sleep 7–8 hours, a regular schedule, and limiting food intake to a 10–12-hour window (mild TRE). Chronic sleep deprivation and cycle shifts worsen steatosis through insulin resistance and cortisol.
🌀
Markers and diagnostics
What to order for a patient with suspected MASLD:
▸ALT, AST, GGT, alkaline phosphatase, total and direct bilirubin, albumin, INR (PT-INR). ▸FIB-4 — a simple noninvasive fibrosis calculator based on age, ALT, AST, and platelets. <1.3 — low risk of advanced fibrosis; >2.67 — high risk (refer to a hepatologist). Updated AASLD 2023 guidelines recommend FIB-4 as primary screening. ▸NFS (NAFLD Fibrosis Score) — an alternative to FIB-4. ▸FibroScan (transient elastography) — measures liver stiffness (kPa) and the controlled attenuation parameter (CAP) for steatosis. Available in outpatient practice. Normal <7 kPa, F4 cirrhosis >12 kPa. ▸MRI-PDFF — the gold standard for quantitative assessment of liver fat. ▸Expanded metabolic panel — HbA1c, fasting insulin, HOMA-IR, lipid panel with sdLDL and ApoB, uric acid, hsCRP. ▸Serologic screening — HBsAg, anti-HCV, ANA, AMA, ceruloplasmin (to exclude viral hepatitis, autoimmune hepatitis, Wilson disease) — mandatory with persistently elevated ALT.
🌀
When to seek care
▸ALT persistently >40 U/L (men) or >19 U/L (women) — see the separate article on healthy ALT limits for more detail ▸FIB-4 >1.3 at any age ▸Liver stiffness on FibroScan >7 kPa ▸Metabolic syndrome, type 2 diabetes, obesity (especially visceral obesity) ▸Family history of cirrhosis or HCC ▸Regular use of “hepatoprotectors” for more than 3 months without objective assessment of effect
I perform a complete metabolic assessment, FIB-4/FibroScan routing, and develop a personalized lifestyle-change protocol with evidence-based nutraceutical support.
🌀
Conclusion
The category of “hepatoprotectors” is a commercial construct, not a clinical reality. Most drugs occupying CIS pharmacy shelves under this label have no RCTs with hard histological endpoints.
The liver in MASLD is treated with weight loss, fructose and alcohol restriction, movement, a Mediterranean diet, coffee, omega-3, choline, and betaine. Among supplements, vitamin E (PIVENS), silymarin (moderately), and NAC have a real evidence base. Among prescription drugs, pioglitazone and semaglutide apply in subgroups.
If after an ALT of 50 U/L a physician prescribes Essentiale and lets the patient go, that is not hepatology; it is routinized market behavior. The real plan is to measure FIB-4, understand the metabolic background, and work with it.
🌀
Sources
▸Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis (PIVENS). *N Engl J Med* 2010;362:1675–1685. PMID 20427778 ▸Loguercio C, Festi D. Silybin and the liver: from basic research to clinical practice. *Drugs* 2012;72:1543–1573. PMID 22994537 ▸Mato JM, Cámara J, Fernández de Paz J, et al. S-adenosylmethionine in alcoholic liver cirrhosis. *J Hepatol* 1999;30:1081–1089. PMID 10579655 ▸Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight loss through lifestyle modification significantly reduces features of NASH. *Gastroenterology* 2015;149:367–378. PMID 25865049 ▸Lindor KD, Kowdley KV, Heathcote EJ, et al. Ursodeoxycholic acid for treatment of nonalcoholic steatohepatitis. *Hepatology* 2004;39:770–778. PMID 15239089 ▸Properzi C, O'Sullivan TA, Sherriff JL, et al. Ad libitum Mediterranean and low-fat diets both significantly reduce hepatic steatosis. *Hepatology* 2018;68:1741–1754. PMID 29476613 ▸Kennedy OJ, Roderick P, Buchanan R, et al. Coffee, including caffeinated and decaffeinated coffee, and the risk of hepatocellular carcinoma. *Aliment Pharmacol Ther* 2017;46:562–574. PMID 28166877 ▸Parker HM, Johnson NA, Burdon CA, et al. Omega-3 supplementation and non-alcoholic fatty liver disease: a systematic review and meta-analysis. *J Hepatol* 2012;56:944–951. PMID 22023985 ▸Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus on a new fatty liver disease nomenclature. *Hepatology* 2023;78:1966–1986. PMID 37363821 ▸Zeisel SH, da Costa KA. Choline: an essential nutrient for public health. *Nutr Rev* 2009;67:615–623. PMID 19906248
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
If my physician prescribed Essentiale, should I stop it? Not on your own. Discuss with your physician what the treatment goals are and which endpoints they want to see (ALT? FibroScan? FIB-4?). If this is MASLD without a specific diagnosis, ask for an alternative plan: FIB-4 assessment, metabolic panel, weight and diet recommendations. Essentiale is unlikely to harm you, but it will not solve the problem either.
Are silymarin and Carsil the same thing? No. Silymarin is a mixture of flavonolignans (silibinin, silicristin, silidianin) from milk thistle. Carsil contains silymarin, but its silibinin dose is low. RCTs used standardized silymarin 420–700 mg with a specified % of silibinin. Read the composition, not the label.
Is vitamin E 800 IU safe? For a patient with biopsy-confirmed MASH without diabetes — yes, according to PIVENS. Long-term high-dose use is debated because of concerns about hemorrhagic stroke and all-cause mortality (Miller ER 2005 meta-analysis). In patients with diabetes and in those taking anticoagulants — only under medical supervision. Use the natural D-α-tocopherol form, not synthetic DL.
Can MASLD be cured completely? Yes — in simple steatosis and MASH without advanced fibrosis, 10% weight loss and lifestyle change can lead to histological regression. In F3 fibrosis and F4 cirrhosis, the goal is to stop progression and reduce HCC risk; complete fibrosis regression is possible, but it takes months and years.
Is coffee really beneficial for a diseased liver? Yes. Epidemiological data are consistent: 2–4 cups/day are associated with a lower risk of cirrhosis and HCC. The effect also applies to decaffeinated coffee. Exceptions include patients with severe insomnia, arrhythmias, or severe GERD.
*This article is for informational purposes and does not replace medical consultation. Before starting any nutraceuticals, changing medication therapy, or undergoing diagnostic procedures, discuss the plan with your treating physician.*
References
- PMID 37363821. PMID 37363821
- PMID 25865049. PMID 25865049
- PMID 20427778. PMID 20427778
- PMID 22994537. PMID 22994537
- PMID 28166877. PMID 28166877
- PMID 10579655. PMID 10579655
- PMID 15239089. PMID 15239089
- PMID 29476613. PMID 29476613
- PMID 16848706. PMID 16848706
- PMID 22023985. PMID 22023985
- Zeisel SH, da Costa KA. Choline: an essential nutrient for public health. Nutr Rev 2009;67:615–623. PMID 19906248