Introduction: bile as a metabolic tool
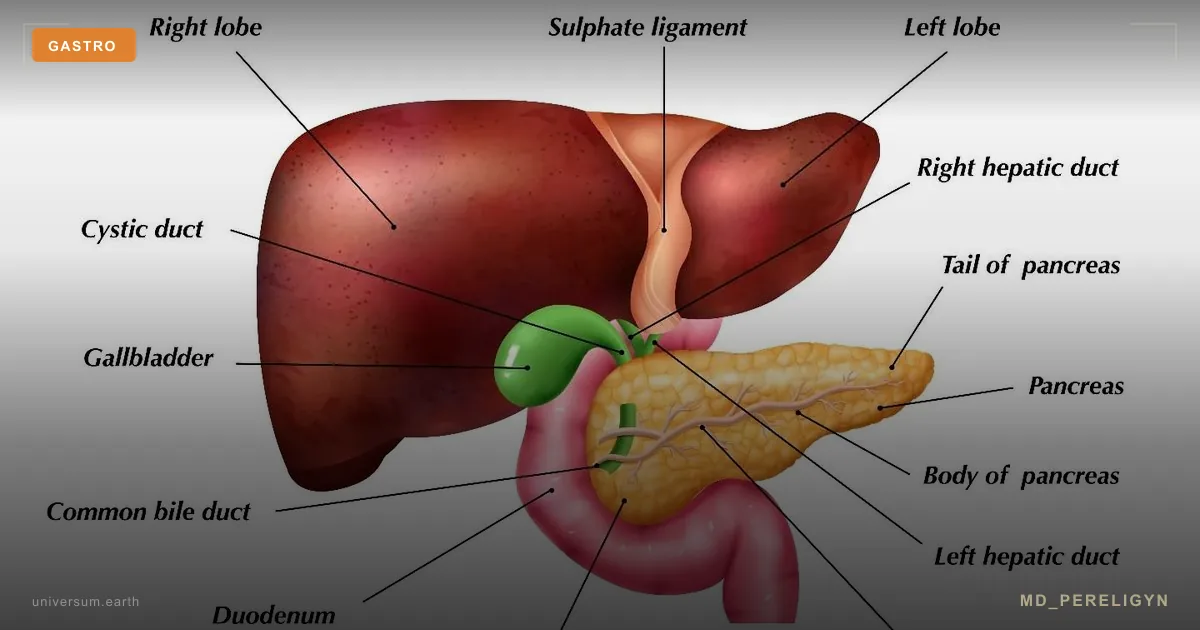
The gallbladder is not an auxiliary sac for fat emulsification. It is part of the enterohepatic circulation, through which the liver eliminates cholesterol, bilirubin, estrogen metabolites, medications, and endogenous toxins. When bile does not flow or becomes thick, not only digestion is impaired, but systemic detoxification as well.
The typical clinical picture is heaviness and dull pain in the right upper quadrant after fatty food, nausea, bitterness in the mouth, bloating, irregular stool, and episodic pain radiating to the right scapula. Ultrasound shows no stones, and the patient is sent home with a diagnosis of “dyskinesia” and generic advice to “avoid fatty foods.”
This misses three underdiagnosed entities: biliary sludge, cholestasis without obstruction, and sphincter of Oddi dysfunction. All three are reversible with proper diagnostics and a protocol. All three can cause dyspepsia, deficiency of fat-soluble vitamins (A, D, E, K), and chronic fatigue through disruption of the microbiota and systemic detoxification.
Key idea of the md_pereligyn protocol: assessment of bile flow is a mandatory part of metabolic screening in patients with insulin resistance, vitamin D deficiency, early osteoporosis, estrogen-dependent conditions, and chronic dyspepsia.
🌀
Physiology: how bile flows
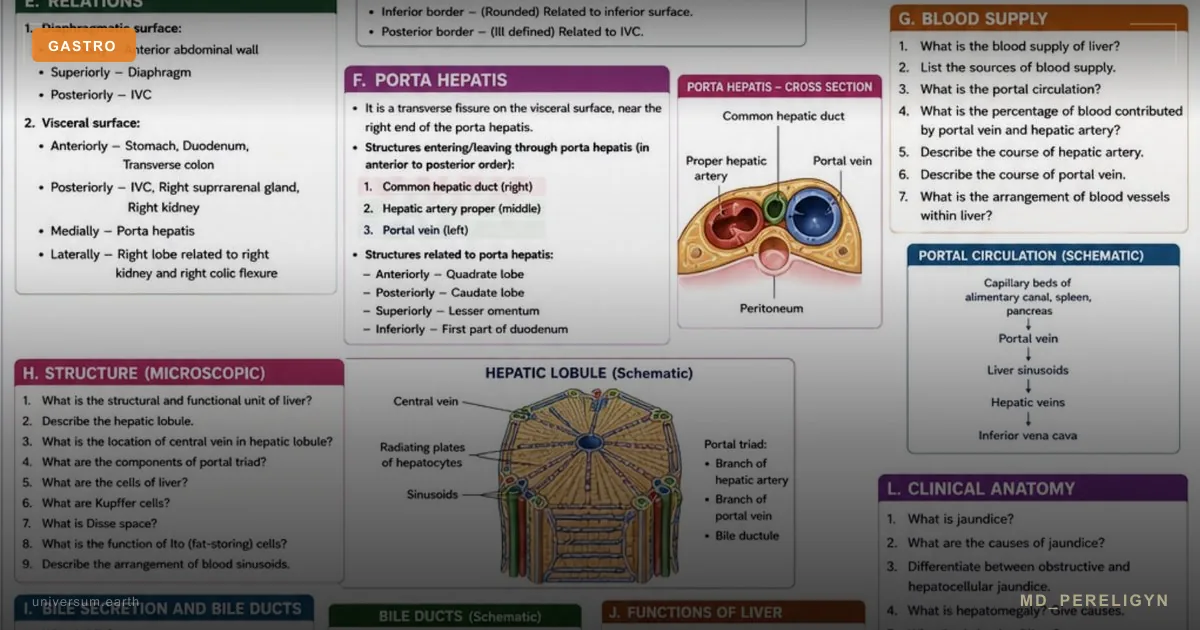
Hepatocytes continuously synthesize 600–1000 ml of bile per day. Composition: water (95%), bile acid salts (cholic, chenodeoxycholic, and their taurine/glycine conjugates), phospholipids (primarily phosphatidylcholine), cholesterol, bilirubin, and electrolytes.
The ratio of bile acids : phospholipids : cholesterol determines whether cholesterol remains in solution or begins to crystallize. This balance is described by the Adler-Schaffer triangle: cholesterol-supersaturated bile is the first step toward sludge and stones.
Between meals, bile is concentrated in the gallbladder 5–10 times. After a meal, cholecystokinin (CCK), released by I-cells of the duodenum in response to fat and amino acids, causes gallbladder contraction and relaxation of the sphincter of Oddi. Bile enters the duodenum, emulsifies fats, and activates pancreatic lipases.
95% of bile acid salts are reabsorbed in the ileum via the ASBT transporter and return to the liver through portal blood. This cycle repeats 6–8 times per day. 5% is lost in stool, which is the main route of cholesterol excretion from the body.
🌀
The sphincter of Oddi and its dysfunction
The sphincter of Oddi is a smooth muscle structure at the junction of the common bile duct, pancreatic duct, and duodenum. Its tone is regulated by CCK (relaxation), VIP, nitric oxide, and the cholinergic system.
Sphincter of Oddi dysfunction (SOD) is spasm or impaired relaxation leading to functional obstruction. Milwaukee classification:
▸Type I — typical biliary pain + ALT/AST/ALP elevated 2-fold during two episodes + common bile duct dilation >12 mm + delayed contrast drainage (>45 min). Best supported by evidence. ▸Type II — biliary pain + one laboratory or imaging criterion. ▸Type III — pain only, without objective criteria. The most controversial category; according to modern data, the effect of sphincterotomy is minimal.
Triggers of dysfunction: cholecystectomy (postcholecystectomy syndrome, up to 30% of patients), chronic stress, estrogen dominance, hypothyroidism, and impaired small-intestinal microbiota.
🌀
Biliary sludge and how it differs from stones
Biliary sludge consists of cholesterol microcrystals and calcium bilirubinates in a mucin matrix. On ultrasound, it appears as hyperechoic sediment without acoustic shadowing. 40% of sludge resolves spontaneously, 20% progresses to stones, and 40% persists chronically.
Stones are the hardened stage. Ultrasound shows hyperechoic structures with acoustic shadowing. Cholesterol stones (80%) result from bile supersaturation with cholesterol. Pigment stones (20%) are associated with hemolysis and infections.
Sludge matters because it more often causes pain and pancreatitis than small stones do, due to migration of microcrystals into the duct and transient obstruction of the sphincter of Oddi. And sludge is precisely the reversible stage where nutritional support works.
🌀
Drivers of cholestasis and sludge
Seven major factors, each of which independently disrupts bile flow:
•Insulin resistance and fatty liver. Fatty infiltration of hepatocytes disrupts secretion of bile acids and phosphatidylcholine. The NAFLD ↔ cholelithiasis association is dose-dependent. •Estrogen dominance. Estrogen increases cholesterol synthesis in bile and reduces its fluidity. Pregnancy, combined oral contraceptives, and HRT are classic triggers. Every additional 5 years of combined oral contraceptive use increases the risk of cholelithiasis by approximately 20%. •Prolonged fasting and intermittent fasting >16 hours. Without gallbladder contraction, bile concentrates and crystallizes. The paradox: what improves insulin sensitivity thickens bile in the absence of choleretic support. •Rapid weight loss. Ketogenic diets, bariatric surgery, and low-calorie protocols. Mobilization of cholesterol from adipose tissue exceeds bile’s capacity to dissolve it, and the risk of stones increases 5–10 times within 6 months. •Hypothyroidism. Thyroid hormones regulate sphincter of Oddi tone and bile acid secretion. Subclinical hypothyroidism is associated with cholelithiasis, especially in women. •Small-intestinal dysbiosis (SIBO). Bacterial deconjugation of bile acids disrupts their reabsorption and increases the toxic fraction of secondary bile acids. •Physical inactivity. Reduced gastrointestinal motility slows gallbladder emptying.
🌀
Markers of cholestasis: what to order
The standard “basic biochemistry” panel with liver enzymes often misses early cholestasis. What actually reflects the state of bile flow:
▸Alkaline phosphatase (ALP) — rises in cholestasis. Target <100 U/L in adults. Isolated ALP elevation suggests cholestasis; together with increased GGT, it indicates hepatic origin; without GGT, bone origin. ▸Gamma-glutamyl transferase (GGT) — the most sensitive marker of the biliary system. Target <30 U/L in men, <20 in women. Rises earlier than ALP. ▸Direct (conjugated) bilirubin — a marker of obstruction at the hepatocyte level and above. Target <0.3 mg/dL. Any elevation is pathological. ▸Total and indirect bilirubin — assessment of hemolysis vs obstruction. ▸ALT, AST — hepatocellular injury. ▸Serum bile acids (fasting and postprandial) — a direct marker of cholestasis, more sensitive than ALP. Fasting reference <10 μmol/L. ▸Fat-soluble vitamins (D, A, E, K-dependent clotting factors, INR) — assessment of malabsorption due to bile deficiency. ▸Hepatobiliary ultrasound with motility assessment (HIDA scan if available). Gallbladder ejection fraction after CCK stimulation <35% indicates hypokinesia. ▸Thyroid panel (TSH, FT4) — mandatory in patients with cholelithiasis and sludge. ▸Estradiol, progesterone, SHBG — in symptomatic women and when estrogen dominance is suspected.
🌀
Holistic protocol for supporting bile flow
The principle of the md_pereligyn protocol: restoring bile flow is not a one-time “detox,” but correction of basic physiology. The strategy includes regular gallbladder emptying, support for bile hydrophilicity, hepatocyte protection, and relief of sphincter of Oddi spasm.
### 1. Hydrophilic bile acids — TUDCA and UDCA
▸UDCA (ursodeoxycholic acid) 10–15 mg/kg/day — the standard treatment for primary biliary cholangitis (Lindor KD, NEJM 2009, PMID 15239089[1]), effective in cholesterol-supersaturated bile and microlithiasis. It dissolves small cholesterol stones (<5 mm) in patients with a functioning gallbladder over 6–12 months. ▸TUDCA (tauroursodeoxycholic acid) 250–750 mg/day — a conjugated form with better bioavailability, supporting hepatocyte function and reducing ER stress. Its evidence base is smaller than that of UDCA, but clinically it is comparable in cholestasis.
UDCA does not work for pigment stones, calcified stones, or absent gallbladder function. Before prescribing it, ultrasound and motility assessment are required.
### 2. Choleretics and cholagogues
Choleretics increase bile synthesis in the liver; cholagogues stimulate gallbladder contraction.
▸Artichoke (Cynara scolymus, extract) 320–640 mg/day — dual action, with evidence for reducing dyspepsia (Holtmann G, Aliment Pharmacol Ther 2003, PMID 14653829[2]). ▸Turmeric (curcumin with piperine or liposomal) 500–1000 mg — a choleretic, reduces inflammation in the biliary tract. Caution in the presence of stones, as it may provoke colic. ▸Milk thistle (silymarin) 200–400 mg/day — hepatoprotection, support for hepatocyte regeneration. ▸Betaine (trimethylglycine) 1500 mg/day — a methyl-group donor, lowers homocysteine, supports phosphatidylcholine synthesis in bile. ▸Choline (bitartrate or alpha-GPC) 500 mg/day — substrate for phosphatidylcholine; choline deficiency is a common cause of “thick” bile. ▸Sunflower lecithin 1–2 tablespoons/day — dietary phosphatidylcholine.
### 3. Relaxation of the sphincter of Oddi
▸Magnesium (glycinate / taurate) 400 mg — a smooth muscle relaxant, reduces sphincter spasm. ▸Peppermint (oil, enteric-coated capsule) 0.2 ml × 3 — antispasmodic effect in the upper gastrointestinal tract (use cautiously in cholelithiasis). ▸Glycine 3 g before meals — antispasmodic, support for phase II detoxification. ▸Stress management — parasympathetic activation (diaphragmatic breathing before meals, slower eating) clinically reduces SOD symptoms.
### 4. Regular gallbladder emptying
Bile should not stagnate. The strategy is 3 meals per day with sufficient fat, without prolonged fasting intervals >14–16 hours in the setting of sludge.
▸Breakfast with fat within one hour after waking — olive oil, avocado, eggs, sardines. This is the first CCK signal and the first emptying. ▸Cold-pressed oils (extra virgin olive oil, avocado oil) — gentle cholagogues. ▸Bitters before meals — arugula, chicory, artichoke, grapefruit (if there are no drug interactions) — stimulate CCK through tongue receptors.
### 5. Basic nutritional support
▸Vitamin D3 + K2 — in cholestasis, malabsorption of fat-soluble vitamins is almost guaranteed. Target 25(OH)D 50–80 ng/mL. ▸Vitamin A (retinol) 5000–10000 IU/day — in confirmed deficiency. ▸Vitamin K2 (MK-7) 100–200 mcg — the cholesterol-K2-calcium axis, protection against arterial calcification. ▸Omega-3 (EPA+DHA) 2 g/day — omega-3 index >8%. Reduces inflammation of the biliary tract and improves membrane fluidity. ▸Vitamin C 500–1000 mg — cofactor for bile acid synthesis. ▸Taurine 1–3 g/day — substrate for bile acid conjugation, reduces the toxicity of secondary bile acids.
### 6. Microbiota and SIBO
SIBO-related deconjugation of bile acids disrupts enterohepatic circulation and sustains cholestasis. With typical symptoms (bloating within the first 30–60 minutes after meals, heartburn, diarrhea/constipation):
▸Lactulose or glucose breath test — SIBO diagnostics. ▸Targeted antimicrobial therapy (rifaximin, if needed with neomycin — physician-prescribed). ▸Postbiotic approach — after eradication: butyrate, fermented foods, slow FODMAP expansion.
🌀
What does NOT work (and why)
▸Prolonged fasting (>16 hours) in the setting of sludge. Bile concentrates without gallbladder contraction and crystallizes. Intermittent fasting can be metabolically useful, but with sludge it requires choleretic support and compensatory “emptying” meals. ▸“Liver flushes” with olive oil and magnesium sulfate. A folk procedure. The “stones” passed in stool are saponified fatty soaps, not real calculi. There is no true duct emptying. In patients with stones, there is a risk of migration and obstruction. ▸Abrupt low-calorie diets and starting keto without bile support. Mobilization of cholesterol from adipose tissue exceeds bile’s dissolving capacity, and new stones form. Before aggressive weight loss: assess ALP, GGT, and ultrasound; if sludge is present, start UDCA or TUDCA at the beginning. ▸Coffee enemas as “liver detox.” There is no evidence base, and there is a risk of electrolyte disturbances and perforation. ▸Self-prescribed UDCA for pigment stones. It does not work and wastes time. ▸Cholecystectomy for “dyskinesia” or type III SOD without objective criteria. Modern data do not support the efficacy of sphincterotomy for a purely pain-based syndrome without laboratory and imaging markers (Cotton PB, JAMA 2014, PMID 24823555[3]).
🌀
When to seek evaluation
▸Heaviness, nausea, or bitterness in the mouth after fatty food more than 2–3 times per week ▸Episodic right upper quadrant pain radiating to the right scapula or shoulder ▸Greasy, pale stool that is difficult to flush (steatorrhea) — a sign of malabsorption ▸Chronic vitamin D deficiency that does not correct with standard doses ▸Postcholecystectomy syndrome with symptom recurrence ▸Early osteoporosis without obvious causes (possible vitamin K deficiency) ▸Resistant dyspepsia that does not respond to PPIs ▸Pregnancy with itching of the palms and soles — exclude intrahepatic cholestasis of pregnancy ▸Rapid weight loss, bariatric surgery, ketogenic diet — preventive assessment
I perform a full hepatobiliary screening (ALP, GGT, direct bilirubin, serum bile acids, ultrasound with motility assessment, HIDA if needed), evaluate the microbiota and thyroid status, and create a personalized bile-flow support protocol — without escalation to surgery where it is not needed.
🌀
Conclusion
The gallbladder is not an auxiliary organ, but part of systemic metabolism and detoxification. Cholestasis and sludge develop years before stones appear and are reversible with proper diagnostics. The strategy of the md_pereligyn protocol: restore regular emptying, increase bile hydrophilicity (TUDCA / UDCA, phosphatidylcholine, taurine), relieve sphincter of Oddi spasm (magnesium, stress management), correct dysbiosis, and remove drivers (insulin resistance, estrogen dominance, hypothyroidism).
Prolonged fasting can be metabolically useful, but with sludge it requires choleretic support. Cholecystectomy is the last step, not the first. In most patients, restoration of bile flow is possible without surgery when the protocol is followed consistently for 3–6 months.
🌀
Sources
▸Lindor KD, Gershwin ME, Poupon R, et al. Primary biliary cirrhosis. *Hepatology* 2009;50:291–308. PMID 15239089 ▸Holtmann G, Adam B, Haag S, et al. Efficacy of artichoke leaf extract in the treatment of patients with functional dyspepsia. *Aliment Pharmacol Ther* 2003;18:1099–1105. PMID 14653829 ▸Cotton PB, Durkalski V, Romagnuolo J, et al. Effect of endoscopic sphincterotomy for suspected sphincter of Oddi dysfunction on pain-related disability. *JAMA* 2014;311:2101–2109. PMID 24823555 ▸Pak M, Lindseth G. Risk factors for cholelithiasis. *Gastroenterol Nurs* 2016;39:297–309. PMID 27467059 ▸Kim H, Im JH, Park S, et al. Subclinical hypothyroidism and risk of cholelithiasis. *World J Gastroenterol* 2018;24:4815–4824. PMID 30479466 ▸Vítek L, Carey MC. New pathophysiological concepts underlying pathogenesis of pigment gallstones. *Clin Res Hepatol Gastroenterol* 2012;36:122–129. PMID 22272472 ▸Vesa CM, Behl T, Nemeth S, et al. Therapeutic role of TUDCA in metabolic and neurodegenerative disorders. *Biomed Pharmacother* 2020;131:110636. PMID 32841839
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
Can I do intermittent fasting with biliary sludge? With caution. Intervals >14 hours without gallbladder contraction concentrate bile. With ultrasound-confirmed sludge, first complete an 8–12 week course of TUDCA or UDCA + choleretic support (artichoke, choline, lecithin), then gradually expand the fasting window. Breakfast with fat within the first hour after waking is mandatory during the active phase.
How is TUDCA different from UDCA? UDCA is the standard with a large evidence base in primary biliary cholangitis and microlithiasis. TUDCA is its taurine-conjugated form; it is better absorbed, supports hepatocyte function, and reduces ER stress. Clinically, they are comparable in cholestasis; when UDCA is available, it makes sense to start with it. Combined use (UDCA in the morning, TUDCA in the evening) is common clinical practice.
What is more important for bile flow — choline or taurine? Choline is needed for phosphatidylcholine synthesis (a bile component that keeps cholesterol in solution). Taurine is needed for bile acid conjugation (increases their hydrophilicity and reduces toxicity). Both are needed. Choline deficiency is common when eggs and liver are restricted; taurine deficiency is seen in vegetarians and patients taking PPIs.
I no longer have a gallbladder — do I need to do anything? Yes. After cholecystectomy, bile flows continuously and the concentration function is lost. Possible issues include bile acid diarrhea, deficiency of fat-soluble vitamins, and postcholecystectomy SOD. Support: fractional meals 5–6 times per day, taurine, choline, lecithin, and if needed, bile acid sequestrants (cholestyramine) for diarrhea. Vitamin D and K2 monitoring is mandatory.
Is it dangerous to take turmeric with gallstones? Curcumin is a powerful cholagogue and provokes gallbladder contraction. If stones >5 mm are present, migration and duct obstruction are possible. With confirmed stones, turmeric should be used only after agreement with a physician and assessment of stone size/number. With sludge but no stones, it is usually safe and useful.
*This article is for informational purposes and does not replace medical consultation. Before starting any nutraceuticals, changing medication therapy, or undergoing diagnostic procedures, discuss the plan with your treating physician.*
References
- PMID 15239089. PMID 15239089
- PMID 14653829. PMID 14653829
- PMID 24823555. PMID 24823555
- Pak M, Lindseth G. Risk factors for cholelithiasis. Gastroenterol Nurs 2016;39:297–309. PMID 27467059
- Kim H, Im JH, Park S, et al. Subclinical hypothyroidism and risk of cholelithiasis. World J Gastroenterol 2018;24:4815–4824. PMID 30479466
- Vítek L, Carey MC. New pathophysiological concepts underlying pathogenesis of pigment gallstones. Clin Res Hepatol Gastroenterol 2012;36:122–129. PMID 22272472
- Vesa CM, Behl T, Nemeth S, et al. Therapeutic role of TUDCA in metabolic and neurodegenerative disorders. Biomed Pharmacother 2020;131:110636. PMID 32841839