Introduction: ferritin is not “stores,” but a signal
In routine practice, ferritin is often interpreted simplistically: low means anemia, high means “good stores.” This is a clinically dangerous oversimplification. Ferritin is an iron-storage protein and also an acute-phase reactant: it rises with inflammation, metabolic syndrome, alcohol intoxication, infections, and malignant disease. It is also an early indicator of true iron overload, which leads to liver fibrosis, cardiomyopathy, arthropathy, and insulin resistance.
The “above normal” threshold beyond which the cause must be investigated is ferritin > 300 μg/L in men and > 200 μg/L in postmenopausal women (AASLD haemochromatosis guidelines, Bacon BR Hepatology 2011, PMID 21452290[1]). This threshold does not mean a diagnosis. It means the physician has a duty to ask: why?
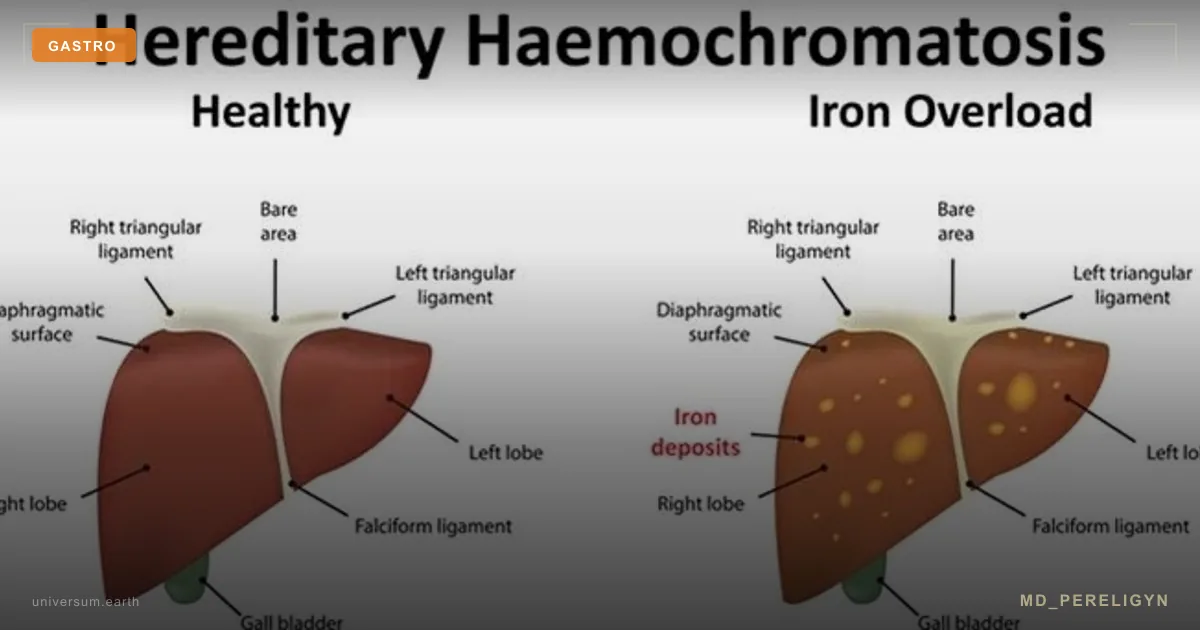
Key point of the md_pereligyn protocol: up to 1 in 200 people of Northern European ancestry are homozygous for the C282Y mutation in the HFE gene, the most common monogenic disease in this population (Adams PC, NEJM 2008, PMID 18510626[2]). Most of them do not know their diagnosis until cirrhosis, diabetes, or cardiomyopathy develops. Timely phlebotomy is a simple, inexpensive, and fully effective intervention if started before the fibrosis phase.
In parallel, in patients with MASLD (metabolic dysfunction-associated steatotic liver disease), ferritin is often mildly elevated, but this is not primary iron overload. Distinguishing these two scenarios is a clinical skill that fundamentally changes management.
🌀
What ferritin is and why it rises
The ferritin molecule is a spherical “capsule” made of 24 subunits that can hold up to 4 500 iron atoms in the form of hydroxyphosphate. This is a safe storage form: free iron is toxic, the ferritin core is not. Ferritin is intracellular, but a small fraction is secreted into plasma and measured in blood tests.
Serum ferritin rises in three main scenarios:
▸True iron overload — hereditary haemochromatosis, repeated blood transfusions, thalassemia, long-term parenteral iron. It is accompanied by increased transferrin saturation (TSAT) > 45% in men and > 40% in women. ▸Systemic inflammation — infections, autoimmune processes, oncology, metabolic syndrome. Ferritin behaves as an acute-phase protein, while TSAT remains normal or reduced. ▸Liver injury — alcoholic hepatitis, MASLD, hepatocellular carcinoma: hepatocytes release ferritin when injured, similarly to ALT.
Therefore, isolated ferritin without TSAT, CRP, ALT, and context is clinically useless. This is the key error in laboratory interpretation.
🌀
Mechanism of iron-induced injury: the Fenton reaction
When the capacity of ferritin and transferrin is exhausted, non-transferrin-bound iron (NTBI) appears in plasma: unbound “free” iron. It enters hepatocytes, cardiomyocytes, pancreatic β-cells, and endocrine organs.
Inside the cell, Fe²⁺ reacts with hydrogen peroxide H₂O₂ through the Fenton reaction:
Fe²⁺ + H₂O₂ → Fe³⁺ + OH• + OH⁻
The hydroxyl radical (OH•) is one of the most reactive oxidants in biology. It damages membrane lipids (lipid peroxidation, LPO), proteins, and DNA. The result: lipid peroxidation, activation of hepatic stellate cells, and fibrosis formation (Pietrangelo A, Gastroenterology 2010, PMID 20149788[3]).
Target organs in descending order of sensitivity: liver → pancreas → myocardium → joints → pituitary → gonads. Clinically, this unfolds as “bronze diabetes,” the classic triad of cirrhosis + diabetes mellitus + bronze skin pigmentation. Today the triad is rare: haemochromatosis is diagnosed before it develops if the physician knows what to look for.
🌀
Drivers of elevated ferritin
Eight causes of ferritin elevation in clinical practice, in order of frequency:
•Metabolic syndrome / MASLD — the most common cause of a “mild” ferritin elevation (300–500 μg/L) in modern practice. Mechanism: hepatocellular inflammation + moderate hepcidin block. TSAT is usually normal (<45%). •Alcohol burden — even moderate consumption (>20 g/day) raises ferritin through CYP2E1 induction and oxidative stress. After 4 weeks of abstinence, ferritin falls by 30–50%. •Hereditary haemochromatosis (HFE C282Y/C282Y or C282Y/H63D) — C282Y homozygosity reaches up to 1:200 in Northern European populations, with phenotype penetrance of 28% in men and 1% in women (Allen KJ, NEJM 2008, PMID 18987254[4]). •Inflammation of any origin — an acute-phase response. Ferritin may be >1000 μg/L in sepsis, Still’s disease, and hemophagocytic syndrome. •Chronic transfusion burden — thalassemia, sickle cell anemia, myelodysplastic syndromes. Each unit of blood = 200 mg of iron. After 20 transfusions, the overload becomes clinically significant. •Parenteral iron in doses exceeding metabolic needs — typical in patients on hemodialysis. •Hepatocellular injury — acute and chronic hepatitis, ischemic hepatitis, drug-induced liver injury. •Malignant disease — Hodgkin lymphoma, HCC, leukemias, neuroblastomas (tumors actively use iron for proliferation).
🌀
Markers: what to order after ferritin
Isolated ferritin is not diagnostic. The minimum investigation panel for ferritin > 300 (men) or > 200 (women):
▸Transferrin saturation (TSAT) = (serum iron / TIBC) × 100%. The main marker of true overload. TSAT > 45% in men, > 40% in women — referral for HFE genotyping. ▸hsCRP — to distinguish an acute-phase elevation from true overload. With inflammation and infection, ferritin ↑, while TSAT is normal or ↓. ▸ALT, AST, GGT — assessment of hepatocellular injury. In haemochromatosis, ALT is often moderately elevated without a pronounced inflammatory response. ▸HFE genotyping (C282Y, H63D, S65C) — when TSAT > 45% and/or there is a family history. A one-time test; genetics for life. ▸Liver MRI T2* — noninvasive quantitative assessment of iron concentration (LIC, liver iron concentration). Normal <1.8 mg Fe / g dry tissue. Replaces biopsy in most patients. ▸FibroScan / ELF / FIB-4 — fibrosis assessment. With LIC > 4 mg/g and F2+ fibrosis, biopsy is indicated for precise staging. ▸HbA1c, fasting insulin — diabetes develops years before clinical overload; early screening is mandatory. ▸Echocardiography — in patients with long-standing overload to assess iron cardiomyopathy.
A detailed discussion of liver markers is in the upcoming article AST/ALT ratio and De Ritis.
🌀
Distinguishing haemochromatosis from MASLD-associated ferritin elevation
This distinction is critical: it determines whether phlebotomy is needed.
▸Primary hereditary haemochromatosis: ferritin 500–5000 μg/L, TSAT > 45% (often > 60–80%), HFE C282Y homozygote or compound C282Y/H63D, MRI T2* shows marked iron accumulation in the liver and often the myocardium/pituitary. Treatment: phlebotomy. ▸MASLD-associated ferritin elevation (DIOS — dysmetabolic iron overload syndrome): ferritin 300–700 μg/L, normal TSAT (<45%), metabolic syndrome, steatosis on ultrasound or MRI-PDFF, absence of HFE mutations. Treatment: weight loss, control of insulin resistance, not first-line phlebotomy.
Prescribing phlebotomy to a patient with MASLD without TSAT > 45% is a clinical error. It does not treat the root cause (insulin resistance) and is not supported by evidence-based medicine.
🌀
Holistic protocol for iron overload
The principle of the md_pereligyn protocol: in true hereditary overload (HFE haemochromatosis with phenotype), phlebotomy is the first and mandatory line. No nutraceutical can replace it. But they can support recovery and reduce oxidative damage.
### 1. Phlebotomy (only with a confirmed phenotype)
▸Induction phase — 1 phlebotomy of 450–500 mL weekly or every 2 weeks until the target ferritin is < 50 μg/L and TSAT < 30%. Duration ranges from 6 months to 2 years depending on baseline burden. ▸Maintenance phase — 2–4 phlebotomies per year lifelong to maintain ferritin at 25–50 μg/L. ▸Monitoring — ferritin and complete blood count before every 4th phlebotomy. ▸Alternative when phlebotomy is contraindicated (severe coronary artery disease, poor venous access): erythrocytapheresis or iron chelators (deferasirox, deferoxamine — usually for transfusional overload).
### 2. Dietary iron management
▸Heme iron (meat, liver) is absorbed at 15–35% regardless of stores. Limit red meat to 1–2 times per week; exclude organ meats during active overload. ▸Non-heme iron (plant-derived) is absorbed at 2–20% and regulated by hepcidin. It does not require strict restriction. ▸Tea and coffee with meals — tannins and polyphenols reduce non-heme iron absorption by 60–70%. Use as a natural chelator. ▸Calcium and dairy products with meals — reduce iron absorption by 30–50%. ▸Avoid iron-fortified foods (cereals, flour with added iron) on labels.
### 3. Vitamin C: critical caution
▸Vitamin C increases non-heme iron absorption 3–4-fold when taken at the same time. With iron overload, do not take vitamin C with meals and do not exceed 100 mg/day. ▸Vitamin C enhances the Fenton reaction in the presence of free iron — a potentially pro-oxidant effect. ▸After ferritin normalizes (<100 μg/L), restrictions can be relaxed.
### 4. Antioxidant protection
▸N-acetylcysteine (NAC) 600–1200 mg — a glutathione precursor that protects hepatocytes from oxidative stress. ▸Silymarin (milk thistle) 140 mg 3×/day — a hepatoprotector with proven antioxidant activity in liver disease. ▸Vitamin E 400 IU/day — a membrane antioxidant (discuss with a physician; use caution with coagulopathy). ▸Curcumin (with piperine) 500 mg 2×/day — binds iron into inactive complexes and has anti-inflammatory effects. ▸Green tea (3–4 cups/day) — EGCG chelates iron and reduces absorption.
### 5. Alcohol and liver nutrition
▸Complete abstinence from alcohol is mandatory in haemochromatosis. Alcohol + iron multiplicatively accelerate fibrosis. ▸Mediterranean / DASH pattern — olive oil, fish, vegetables, legumes, nuts. Reduces inflammation and insulin resistance. ▸Restriction of fructose and fast carbohydrates — reduces liver steatosis and systemic inflammation.
### 6. Family screening
▸When HFE C282Y homozygosity is confirmed in a patient, screen all siblings and children. Early detection before phenotype = life without consequences. ▸Minimum: ferritin + TSAT at age 18 in offspring of a homozygote. ▸HFE genotyping in relatives — from age 18 (ethical point: before this age, the mutation does not change management).
🌀
What does NOT work (and why)
▸“Treating high ferritin” without TSAT and context — confusing an acute-phase response with overload. Prescribing phlebotomy for MASLD-associated ferritin elevation is a common mistake. ▸Isolated iron chelators (deferasirox) for HFE haemochromatosis — not first line, more expensive, hepatotoxic, indicated only when phlebotomy is contraindicated. ▸High-dose vitamin C during active overload — increases iron absorption and the Fenton reaction. ▸“Liver cleansing” with supplements without diagnostics — time is lost before fibrosis and cirrhosis develop. ▸Ignoring family history — a missed opportunity for early diagnosis in relatives before phenotype. ▸Lactoferrin and “reducing inflammation” in true overload — do not replace phlebotomy and do not reduce tissue iron stores.
🌀
When to seek care
▸Ferritin > 300 μg/L (men) or > 200 μg/L (postmenopausal women) on repeated tests ▸Ferritin > 1000 μg/L — regardless of sex and context, requires immediate investigation ▸TSAT > 45% (men) or > 40% (women) — referral for HFE genotyping ▸Family history of haemochromatosis, cirrhosis of unknown etiology, early diabetes, or arthropathy ▸Northern European ancestry + unexplained fatigue, arthralgia in the metacarpophalangeal joints of the 2nd and 3rd fingers ▸MASLD + elevated ferritin — to differentiate DIOS from primary haemochromatosis
I perform the full investigation panel (ferritin, TSAT, HFE genotyping, MRI T2* when indicated, FibroScan) and create a personalized plan: phlebotomy and/or metabolic correction depending on the diagnosis.
🌀
Conclusion
Ferritin is not a marker of “enough iron”. It is an acute-phase protein and an indicator of possible overload. Interpreting it in isolation is clinically dangerous.
True hereditary haemochromatosis is the most common monogenic disease in Northern Europeans and, at the same time, one of the easiest to treat if caught before fibrosis. Phlebotomy is an inexpensive and fully effective intervention. The cost of missing it is cirrhosis, diabetes, cardiomyopathy, and a 15–20-year reduction in lifespan.
MASLD-associated ferritin elevation is a different clinical scenario. Treatment is weight loss and metabolic correction, not bloodletting.
Distinguishing these two scenarios is the physician’s task, not the laboratory’s.
🌀
Sources
▸Bacon BR, Adams PC, Kowdley KV, et al. Diagnosis and management of hemochromatosis: 2011 practice guideline by the AASLD. *Hepatology* 2011;54:328–343. PMID 21452290 ▸Adams PC, Barton JC. Haemochromatosis. *Lancet* 2007;370:1855–1860. PMID 18510626 ▸Pietrangelo A. Hereditary hemochromatosis: pathogenesis, diagnosis, and treatment. *Gastroenterology* 2010;139:393–408. PMID 20149788 ▸Allen KJ, Gurrin LC, Constantine CC, et al. Iron-overload-related disease in HFE hereditary hemochromatosis. *N Engl J Med* 2008;358:221–230. PMID 18987254 ▸Powell LW, Seckington RC, Deugnier Y. Haemochromatosis. *Lancet* 2016;388:706–716. PMID 26975792
Related articles: Endothelium: the Foundation of Vascular Health, Cholesterol Without Statins.
🌀
FAQ
If my ferritin is high, do I need phlebotomy immediately? No. First, the cause must be established. At minimum: transferrin saturation (TSAT), hsCRP, ALT, AST, and context. Phlebotomy is indicated only in true overload (TSAT > 45% + elevated ferritin or confirmed HFE phenotype). In MASLD or inflammation, phlebotomy does not treat the root cause.
What should I do if the HFE genotype is C282Y homozygous but ferritin is normal? This is the pre-phenotype phase. 70% of women and about 50% of men with C282Y/C282Y will never develop clinically significant overload. Management: ferritin and TSAT monitoring every 1–2 years, a diet with limited heme iron, alcohol abstinence, and screening of relatives. Phlebotomy is not needed until ferritin rises.
Can I eat meat with haemochromatosis? Yes, but in moderate amounts (1–2 times per week, portions of 80–120 g). Complete avoidance is usually unnecessary. Only organ meats (liver, kidneys) and vitamin C with meals are excluded. Tea and coffee tannins with meals reduce iron absorption.
Is blood donation effective instead of phlebotomy? Yes. With confirmed haemochromatosis, blood can be donated as a regular donor, subject to hemoglobin and interval restrictions. This is therapeutically equivalent to phlebotomy and socially useful. Many blood centers know the indication “haemochromatosis” and accept donations more frequently than standard intervals.
How long do people live with haemochromatosis? With early diagnosis (before fibrosis) and regular phlebotomy, life expectancy does not differ from the general population. When diagnosed at the stage of cirrhosis or diabetes, median survival falls by 5–15 years. Timeliness is the key factor.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 21452290. PMID 21452290
- PMID 18510626. PMID 18510626
- PMID 20149788. PMID 20149788
- PMID 18987254. PMID 18987254
- Powell LW, Seckington RC, Deugnier Y. Haemochromatosis. Lancet 2016;388:706–716. PMID 26975792