Introduction: the silence of the liver
The liver is a parenchymal organ with no pain receptors in the tissue itself. Pain appears only when Glisson’s capsule is stretched (a mass lesion, hepatomegaly), in cholestasis with distension of the bile ducts, or in peritonitis. Steatosis, MASH, and F1–F3 fibrosis are asymptomatic.
This means the window into liver status is blood biochemistry. And the main number in that biochemistry is ALT (alanine aminotransferase), an enzyme specific to hepatocytes. An ALT increase means liver cell injury, and its magnitude roughly correlates with injury activity.
The problem is that the upper ALT limit printed on laboratory reports — 40 U/L, or even 45–50 — is a statistical artifact. It was established in the 1980s in populations that already included widespread fatty liver disease and undiagnosed hepatitis C. According to the strict data from Prati et al. (Ann Intern Med 2002, PMID 12027555[1]), the true upper ALT limit is 30 U/L in men and 19 U/L in women.
Key thesis of the md_pereligyn protocol: ALT 25–40 U/L in a non-drinking person without viral hepatitis is not normal. It is a signal of silent MASLD that most physicians miss. Missing this stage turns, over 10–15 years, into fibrosis, cirrhosis, and HCC — endpoints that could have been avoided.
🌀
What ALT is and why it matters so much
ALT (alanine aminotransferase) is an intracellular enzyme whose concentration in the hepatocyte is 3000 times higher than in plasma. When the hepatocyte membrane is damaged (from any cause — steatosis, inflammation, a drug, a virus, alcohol), ALT enters the bloodstream and its plasma concentration rises.
ALT is much more liver-specific than AST (which is also present in skeletal muscle, myocardium, and erythrocytes). Therefore, the primary marker when assessing liver injury is ALT.
ALT dynamics: ▸Acute hepatitis (viral, drug-induced, ischemic) — ALT may rise 10–100 times above normal (>1000 U/L). ▸Chronic MASLD/MASH — ALT remains in the 25–80 U/L range for weeks and months. ▸Cirrhosis with hepatocyte depletion — ALT may paradoxically become “normal” or even low because the cells have already died. This is a trap.
🌀
Why “40 is normal” is a myth
In 2002, Prati et al. performed a simple but pivotal analysis. They took a cohort of healthy blood donors without risk factors (normal BMI, normal lipids, negative anti-HCV, negative HBsAg, no alcohol) and recalculated the 95th percentile for ALT.
Result: ▸Men — 95th percentile ALT = 30 U/L. ▸Women — 95th percentile ALT = 19 U/L.
They also showed that patients with ALT in the 30–40 U/L range have a significantly higher risk of histologically confirmed fatty liver disease and metabolic syndrome than patients with ALT <30.
Since then, updated guidelines (ACG Clinical Guideline, Kwo PY, Am J Gastroenterol 2017, PMID 28045128[2]) have officially recommended using lower upper limits: 33 in men and 25 in women (at minimum). EASL and AASLD also recognize that the “40 U/L normal” threshold is historically overestimated.
However, in most laboratories in the CIS, the upper ALT limit is still listed as 40 U/L or higher. This means that millions of patients with real MASLD receive a report where their ALT is marked as “within normal limits” and leave without evaluation.
🌀
Drivers of elevated ALT
The eight most common causes of “slightly elevated ALT” in an asymptomatic person:
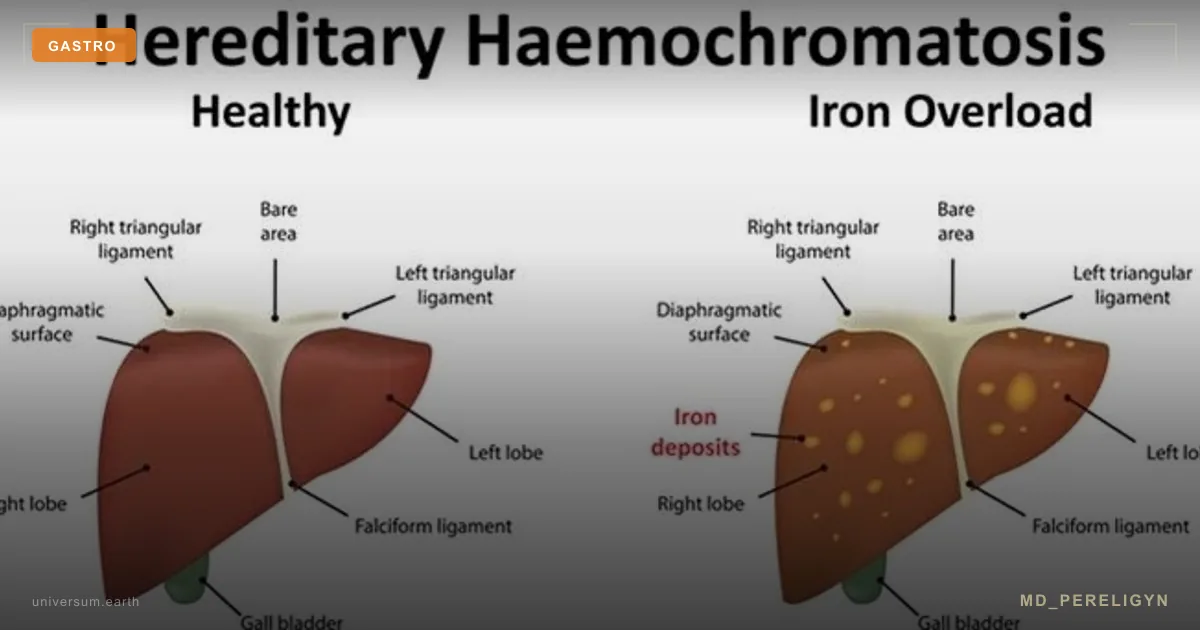
•MASLD/MASH — #1 worldwide. 30% of the adult population, 50–70% with obesity and type 2 diabetes. Visceral fat, insulin resistance, fructose, physical inactivity. •Alcohol — even “moderate” intake (1–2 servings/day regularly) increases ALT and GGT. The toxicity threshold is lower in women than in men. •Drug-induced liver injury (DILI) — statins, paracetamol/acetaminophen (especially >2 g/day chronically), amiodarone, methotrexate, antibiotics (amoxicillin-clavulanate, isoniazid), NSAIDs, valproate, diclofenac, supplements (high-dose green tea EGCG, kava, Iberogast). •Viral hepatitis B and C — must be excluded serologically (HBsAg, anti-HCV) when ALT is persistently elevated. •Autoimmune hepatitis — especially in middle-aged women; markers: ANA, ASMA, anti-LKM, IgG. •Hemochromatosis — hereditary iron accumulation; markers are ferritin and transferrin saturation. •Wilson disease — rare but dangerous; ceruloplasmin and urinary copper, especially in young patients. •Celiac disease — elevated ALT may be the only manifestation. •Hypothyroidism — subclinical and overt forms can cause a moderate ALT increase. •Muscle load — intense training, especially strength training, increases AST and (to a lesser degree) ALT. For differentiation — creatine kinase (CK).
🌀
What to order: the liver assessment panel
Minimum biochemistry for “slightly elevated ALT”:
▸ALT, AST, GGT, alkaline phosphatase (ALP), total and direct bilirubin, albumin, total protein — the initial liver panel. ▸AST/ALT ratio (De Ritis ratio) — <1 in MASLD/MASH, >1 in alcoholic liver disease and cirrhosis, >2 in acute alcoholic hepatitis. ▸GGT — increases with alcohol, cholestasis, and drug-induced enzyme induction. Isolated GGT elevation with normal ALP is often an alcohol signal. ▸Platelets — a decrease <150 × 10⁹/L combined with elevated ALT is a signal of portal hypertension and advanced fibrosis. ▸INR (PT-INR), albumin — hepatic synthetic function; impaired in cirrhosis.
Etiology screening (if ALT is persistently elevated): ▸HBsAg, anti-HCV — mandatory for everyone. ▸Ferritin, transferrin saturation — hemochromatosis. ▸ANA, ASMA, anti-LKM-1, IgG — autoimmune hepatitis. ▸AMA — primary biliary cholangitis (especially with a cholestatic pattern). ▸Ceruloplasmin, 24-hour urinary copper — Wilson disease in young patients. ▸Tissue transglutaminase antibodies (tTG-IgA), total IgA — celiac disease. ▸TSH, free T4 — hypothyroidism. ▸α1-antitrypsin — deficiency as a rare cause.
Metabolic panel: ▸HbA1c, fasting insulin, fasting glucose, HOMA-IR. ▸Advanced lipid panel — ApoB, sdLDL, Lp(a), triglycerides. ▸hsCRP, uric acid.
🌀
Non-invasive fibrosis assessment
Liver biopsy is the gold standard, but it is invasive. Modern non-invasive tests (NITs) allow fibrosis assessment without biopsy in most patients:
▸FIB-4 — a simple calculator based on age, ALT, AST, and platelets. Available online or calculated manually: FIB-4 = (age × AST) / (platelets × √ALT). Interpretation: ▸<1.3 (or <2.0 in patients >65 years) — low risk of significant fibrosis, repeat in 1–3 years. ▸1.3–2.67 — gray zone, additional testing is needed (FibroScan, ELF). ▸>2.67 — high risk of significant fibrosis, refer to a hepatologist. ▸NFS (NAFLD Fibrosis Score) — includes age, BMI, diabetes, AST, ALT, platelets, and albumin. ▸ELF (Enhanced Liver Fibrosis) — a biomarker based on HA, PIIINP, and TIMP-1. Available in major centers. ▸FibroScan (transient elastography) — measures liver stiffness (LSM, kPa) and steatosis (CAP, dB/m). Normal LSM <7 kPa, F2 fibrosis 7–10, F3 — 10–13, F4 (cirrhosis) >13. ▸MRI elastography (MRE) — the most accurate non-invasive method, but expensive and available only in major centers. ▸MRI-PDFF — the gold standard for quantitative assessment of liver fat, recommended for research and difficult cases.
Modern screening pathway (AASLD/EASL 2023): any patient with MASLD risk factors (type 2 diabetes, obesity, metabolic syndrome) → FIB-4 → if FIB-4 >1.3 → FibroScan → if stiffness >8 kPa → refer to a hepatologist.
🌀
Holistic protocol for “silent” MASLD
If ALT is persistently in the 25–60 U/L range without a clear extrahepatic cause, and FIB-4 shows low risk, the protocol is built on the metabolic foundation:
### 1. Metabolism
▸Weight loss of 7–10% from baseline — histologically confirmed regression of MASH (Vilar-Gomez E, Gastroenterology 2015, PMID 25865049[3]). ▸Mediterranean or low-carbohydrate diet — both outperform low-fat diets in their effect on steatosis (Properzi C, Hepatology 2018, PMID 29476613[4]). ▸Restriction of fructose and sweetened beverages — fructose directly stimulates de novo lipogenesis in hepatocytes. ▸Alcohol — abstinence in confirmed MASH/fibrosis; limitation to 1 serving/day in women and 2 in men with simple steatosis.
### 2. Movement
▸Aerobic exercise 150 min/week + strength training 2–3 times/week — reduces steatosis even without weight loss.
### 3. Coffee
▸Coffee 2–4 cups/day — a consistent association with lower risk of cirrhosis and HCC (Kennedy OJ, Aliment Pharmacol Ther 2017, PMID 28166877[5]). The effect also applies to decaffeinated coffee.
### 4. Choline and methylation
▸Choline 425 mg (women) / 550 mg (men) — dietary reference intake. Choline deficiency in humans causes steatosis within 6 weeks (Zeisel SH). ▸Betaine 1500–3000 mg/day — a methyl group donor. ▸Vitamins B6, B9 (methylfolate), B12 — methylation cofactors.
### 5. Targeted supplements (after assessment)
▸Vitamin E (D-α-tocopherol) 400–800 IU — in NON-diabetic patients with biopsy-confirmed MASH (PIVENS, Sanyal 2010, PMID 20427778[6]). ▸Silymarin (standardized) 420–700 mg/day — moderate benefit. ▸EPA+DHA 2–4 g/day — reduction of liver fat (Parker HM, J Hepatol 2012, PMID 22023985[7]). ▸N-acetylcysteine (NAC) 600 mg twice daily — a glutathione precursor.
### 6. Review of medication burden
▸Audit all medications and supplements being taken. Remove hepatotoxic candidates where possible (especially meaningless “hepatoprotectors,” excessive NSAIDs, and excessive doses of green tea).
### 7. Vitamin D and sleep
▸Vitamin D3 to 40–60 ng/mL. ▸Sleep 7–8 hours, regular schedule, 10–12-hour eating window.
🌀
What does NOT work (silent MASLD traps)
▸“Normal ALT 38 U/L = everything is fine” — no, especially in women (above 19 is already a signal) and in the presence of metabolic factors. ▸“I’ll prescribe Essentiale and forget about it” — without FIB-4 assessment, without excluding viruses, and without lifestyle work, this is simulated treatment; see the separate article on hepatoprotectors. ▸“ALT normalized — the disease is gone” — no. ALT may normalize with hepatocyte depletion (advanced fibrosis/cirrhosis), and also when inflammatory activity decreases while steatosis and fibrosis persist. FIB-4 and FibroScan monitoring are more important than ALT. ▸Ignoring isolated elevated GGT — often a signal of alcohol use that the patient hides or underestimates. ▸Liver cleanses, tubage, monastery tea — there is no evidence that these interventions improve outcomes in MASLD.
🌀
When to seek care
▸ALT persistently >30 U/L (men) or >19 U/L (women) on two measurements 4–8 weeks apart ▸ALT >2× the upper limit of normal — a full etiologic panel is mandatory ▸FIB-4 >1.3 at any age ▸Liver stiffness on FibroScan >7 kPa ▸Metabolic syndrome, type 2 diabetes, obesity (especially visceral) ▸Family history of cirrhosis or HCC ▸Systematic use of drugs with known hepatotoxicity ▸Any doubts after several visits where you were told “everything is normal”
I perform a complete metabolic and liver assessment (ALT, AST, GGT, FIB-4, FibroScan routing, serology, metabolic panel) and develop a personalized protocol.
🌀
Conclusion
ALT is the main window into the liver’s silent dynamics. And this window opens earlier than the upper limit printed on the laboratory report. The true thresholds are 30 U/L in men and 19 U/L in women (Prati 2002, ACG 2017).
In an asymptomatic person, “slightly elevated” ALT is not normal. It is either MASLD, alcohol, drug-induced injury, or one of the less common causes that must be excluded (viruses, autoimmune disease, hemochromatosis, Wilson disease, celiac disease).
Pathway: repeat ALT in 4–8 weeks → exclude viral hepatitis → assess FIB-4 → if FIB-4 >1.3, perform FibroScan → if elevation persists, refer to a hepatologist. And always work on the metabolic foundation.
The liver is silent. Tests are its voice. You need to listen carefully.
🌀
Sources
▸Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. *Ann Intern Med* 2002;137:1–10. PMID 12027555 ▸Kwo PY, Cohen SM, Lim JK. ACG Clinical Guideline: Evaluation of abnormal liver chemistries. *Am J Gastroenterol* 2017;112:18–35. PMID 28045128 ▸Sanyal AJ, Chalasani N, Kowdley KV, et al. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis (PIVENS). *N Engl J Med* 2010;362:1675–1685. PMID 20427778 ▸Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L, et al. Weight loss through lifestyle modification significantly reduces features of NASH. *Gastroenterology* 2015;149:367–378. PMID 25865049 ▸Properzi C, O'Sullivan TA, Sherriff JL, et al. Ad libitum Mediterranean and low-fat diets both significantly reduce hepatic steatosis. *Hepatology* 2018;68:1741–1754. PMID 29476613 ▸Kennedy OJ, Roderick P, Buchanan R, et al. Coffee and risk of hepatocellular carcinoma. *Aliment Pharmacol Ther* 2017;46:562–574. PMID 28166877 ▸Parker HM, Johnson NA, Burdon CA, et al. Omega-3 supplementation and non-alcoholic fatty liver disease: a meta-analysis. *J Hepatol* 2012;56:944–951. PMID 22023985 ▸Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus on a new fatty liver disease nomenclature. *Hepatology* 2023;78:1966–1986. PMID 37363821 ▸European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis. *J Hepatol* 2021;75:659–689. PMID 34166721
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
My ALT is 35 and my doctor says “everything is normal.” What should I do? Repeat the test in 4–8 weeks in the same laboratory, in the morning while fasting, with no intense training for 48 hours beforehand. If it remains persistently >30 (men) / >19 (women), ask for at least HBsAg, anti-HCV, GGT, ferritin, TSH, HbA1c, fasting insulin, an advanced lipid panel, and FIB-4 calculation. If the physician refuses, see a hepatologist or gastroenterologist.
I train, and my ALT is 50. Is it from exercise? Partly possible, especially with strength training 48–72 hours before the test. But “blaming everything on sport” is a trap. Repeat the test after 72 hours of rest from intense exercise. Also measure CK (creatine kinase) — if it is substantially elevated and AST is higher than ALT, the source is more likely muscular. If ALT remains elevated with low CK, the origin is hepatic.
My FIB-4 is 0.9 — does that mean everything is normal? Not exactly. FIB-4 is good at excluding advanced fibrosis (F3–F4), but it does not exclude simple steatosis or MASH. If you have metabolic factors (obesity, diabetes, dyslipidemia), it is worth doing FibroScan or at least liver ultrasound, and most importantly, working on lifestyle.
Can I drink alcohol with MASLD? With simple steatosis without fibrosis — limited intake (no more than 1 serving/day in women, 2 in men, and 2–3 alcohol-free days per week). With confirmed MASH/fibrosis — abstinence from alcohol, because alcohol and MASLD synergistically accelerate progression.
How long does it take for ALT to normalize after lifestyle change? In simple steatosis with 5–7% weight loss, ALT usually normalizes within 8–16 weeks. In MASH, it is slower: 6–12 months. It is important to understand that ALT normalization ≠ complete cure; FIB-4 and FibroScan monitoring are more important.
*This article is informational and does not replace medical consultation. Before starting any nutraceuticals, changing medication therapy, or undergoing diagnostic procedures, discuss the plan with your treating physician.*
References
- PMID 12027555. PMID 12027555
- PMID 28045128. PMID 28045128
- PMID 25865049. PMID 25865049
- PMID 29476613. PMID 29476613
- PMID 28166877. PMID 28166877
- PMID 20427778. PMID 20427778
- PMID 22023985. PMID 22023985
- Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus on a new fatty liver disease nomenclature. Hepatology 2023;78:1966–1986. PMID 37363821
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol 2021;75:659–689. PMID 34166721