Introduction: apnea as an arrhythmia factor
When atrial fibrillation is first documented in a patient (AFib — atrial fibrillation), the standard pathway is antiarrhythmic therapy, anticoagulation, and catheter ablation when indicated. But this pathway often omits one step that determines the entire long-term outcome: screening for obstructive sleep apnea (OSA — obstructive sleep apnea).
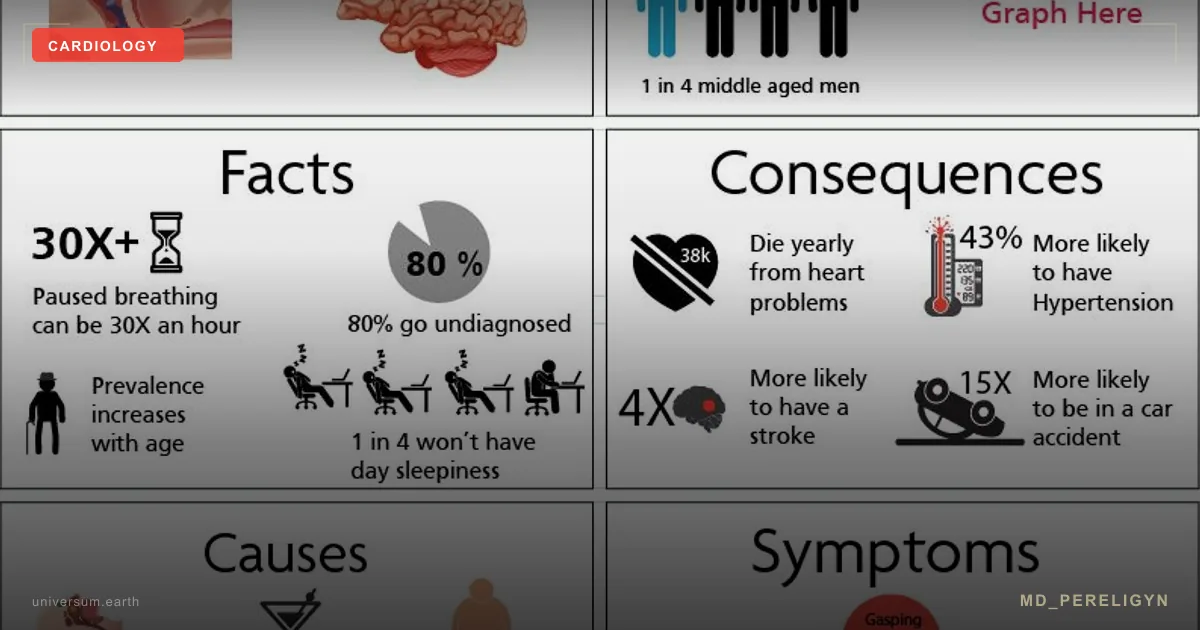
Obstructive sleep apnea is recurrent collapse of the upper airway during sleep, accompanied by episodes of hypoxia, hypercapnia, and microarousals. Each episode triggers a cascade: sympathetic storm → blood pressure spike → intrathoracic pressure swings → stretching of the pulmonary veins and left atrium → triggered activity.
Key point of the md_pereligyn protocol: up to 50% of patients with newly diagnosed AFib have undiagnosed OSA. Without correction of OSA, ablation is followed by AFib recurrence within one year in 60–80% of cases. With CPAP therapy (continuous positive airway pressure), this falls to 30–40%.
In other words: treating arrhythmia without treating sleep is an attempt to stop a forest fire without turning off the arsonist. The fire will flare up again and again.
🌀
Mechanism: how OSA creates AFib
The OSA → AFib link is not merely a statistical correlation. It is specific pathophysiology described in dozens of experimental and clinical studies:
▸Hypoxia (SpO₂ falls to 80–85% and below) → sympathetic activation → increased atrial automaticity and shortening of the refractory period. ▸Hypercapnia (CO₂ rises between apneas) → chemoreceptor activation → paradoxical “vagal surge” when breathing resumes → shortening of the atrial refractory period. ▸Intrathoracic pressure swings (inspiratory efforts against a closed airway generate pressure down to −60 cm H₂O) → stretching of the pulmonary veins and left atrium → triggered activity from the pulmonary vein ostia, the very source targeted by catheter ablation. ▸Abrupt blood pressure spikes on arousal → repeated baroreflex activation → atrial myocardial hypertrophy. ▸Chronic inflammation and oxidative stress (increased TNF-α, IL-6, hsCRP) → atrial fibrosis → formation of a substrate for re-entry. ▸Endothelial dysfunction — cyclic hypoxia reduces NO bioavailability, increases ADMA, and accelerates atherosclerosis of the coronary arteries and the atrial myocardial microcirculation.
Thus, OSA simultaneously creates both the trigger (pulmonary vein stretch) and the substrate (atrial fibrosis) for AFib. This is a unique combination, which is why its effect on arrhythmogenesis is multiplicative, not additive.
🌀
Bidirectional relationship
The OSA and AFib relationship works in both directions:
•OSA → AFib: untreated OSA doubles the risk of incident AFib (Gami AS, J Am Coll Cardiol 2007, PMID 17719466[1]). Among patients with severe OSA (AHI ≥30), up to 60% will develop AFib within 10 years. •AFib → OSA: the strong association also works in reverse through pulmonary venous volume overload and chronic inflammation. In patients with long-standing AFib, OSA prevalence is higher than in the general population even with normal BMI. •Recurrence after ablation: in the study by Patel D et al. (Circ Arrhythm Electrophysiol 2010, PMID 20631252[2]), 5-year AFib recurrence after catheter ablation was 78% in patients with untreated OSA versus 39% in patients on CPAP. The absolute difference was 39 percentage points. •Antiarrhythmic efficacy: propafenone, flecainide, and amiodarone work substantially worse in patients with untreated OSA. Any rhythm control strategy loses clinical meaning without apnea correction.
🌀
Screening: the STOP-BANG questionnaire
The most validated screening tool worldwide is the 8-item STOP-BANG questionnaire. Each positive item = 1 point.
▸S — Snoring (loud snoring audible through a closed door) ▸T — Tired (daytime sleepiness, morning fatigue, falling asleep while driving) ▸O — Observed apnea (witnessed breathing pauses during sleep) ▸P — Pressure (hypertension or antihypertensive therapy) ▸B — BMI > 35 kg/m² ▸A — Age > 50 years ▸N — Neck > 40 cm (neck circumference) ▸G — Gender male
Interpretation: •0–2 points — low risk of OSA •3–4 points — intermediate risk; further evaluation is indicated •5–8 points — high probability of OSA; polysomnography or home respiratory polygraphy is indicated immediately
The sensitivity of STOP-BANG ≥3 points for severe OSA is 93%, with specificity of 43%. Low specificity is not a bug but a feature: the cost of missing OSA in a patient with AFib is far higher than the cost of one additional diagnostic study.
🌀
Do NOT confuse it with simple snoring
Not every snore = OSA. The key distinction:
▸Simple snoring — no apnea (breathing pauses), no significant desaturation, no daytime sleepiness, no cardiovascular consequences. A social problem, not a medical one. ▸OSA — breathing pauses ≥10 seconds, AHI (apnea-hypopnea index) ≥5 events/hour on polygraphy, desaturation ≥3%, or microarousals. A medical diagnosis with prognostic implications.
Severity by AHI: •AHI 5–14 — mild OSA •AHI 15–29 — moderate OSA •AHI ≥30 — severe OSA (often with desaturations to 80% and below)
In a patient with AFib, AHI ≥15 is an indication for CPAP therapy before and after ablation. This is not “optional”; it changes the long-term outcome.
🌀
Holistic protocol
CPAP is the standard, but it is not the only tool. The md_pereligyn protocol is built in three levels.
### 1. Diagnosis and baseline therapy
▸Polysomnography (PSG) — the gold standard, performed in a sleep laboratory. EEG, EOG, EMG, ECG, breathing, SpO₂, and leg movements are recorded. ▸Home sleep apnea testing (HSAT) — a simplified option for patients with a high pretest probability of OSA. It is sufficient for diagnosis when AHI ≥15. ▸CPAP for AHI ≥15 or AHI 5–14 with symptoms / concomitant CVD. Modern devices are auto-CPAP (APAP); the mask is selected individually. Adherence is monitored through the manufacturer’s app (≥4 h/night, ≥70% of nights). ▸Alternatives to CPAP when CPAP is not tolerated: oral appliances (mandibular advancement device — MAD) for AHI <30; hypoglossal nerve stimulation (Inspire) in selected candidates.
### 2. Metabolic foundation
In most cases, OSA is a consequence of metabolic syndrome and visceral obesity. Without addressing the foundation, CPAP suppresses the symptom but does not remove the cause.
▸Weight reduction by 7–10% from baseline — may reduce AHI by 30–50% and restore rhythm in some patients with mild to moderate OSA. ▸Strength training 2–3 times/week — increases lean mass and improves insulin sensitivity. ▸Aerobic activity 150 min/week — reduces visceral fat, a key source of inflammatory cytokines. ▸HbA1c control <5.7% — hyperglycemia amplifies atrial fibrosis. ▸Mediterranean / DASH pattern — olive oil, fish, vegetables. Reduction of systemic inflammation.
### 3. Correction of factors that worsen OSA
▸Alcohol <14 g/day in men, <7 g/day in women, and avoid for 3–4 hours before sleep — ethanol relaxes pharyngeal muscles and deepens apnea. ▸Review benzodiazepines and Z-drugs (zolpidem) — they worsen OSA and increase AHI by 20–30%. Consider substitution with trazodone, melatonin, or ramelteon for insomnia. ▸Opioids — increase central apneas; analgesia should be reviewed in chronic pain. ▸Smoking — pharyngeal mucosal edema, a direct OSA trigger. ▸Avoid supine sleep (positional therapy — a tennis ball in a pocket on the back of pajamas; modern wearable devices). In 30% of patients, AFib is positional. ▸ENT consultation — enlarged tonsils, septal deviation, and soft palate hypertrophy may require surgical correction (UPPP, septoplasty, tonsillectomy).
### 4. Support of the atrial myocardium
▸Magnesium (glycinate / taurate) 400 mg/day — antiarrhythmic effect and support of insulin sensitivity. ▸Potassium 4–5 g/day through diet — leafy greens, avocado, legumes. ▸Omega-3 (EPA+DHA) 2 g/day — reduction of atrial fibrosis; target omega-3 index >8%. ▸CoQ10 (ubiquinol) 100–200 mg/day — support of myocardial mitochondrial function. ▸Vitamin D3 to a level of 60–80 ng/mL — deficiency is associated with AFib progression.
🌀
What does NOT work (and why)
▸Ablation without OSA screening — in a patient with severe untreated OSA, AFib recurrence after one year is 60–80%. The ablation succeeded technically; biology won. ▸Antiarrhythmics with untreated OSA — propafenone, flecainide, and sotalol work substantially worse. Doses are escalated, adverse effects increase, and the effect remains minimal. ▸“I have snored all my life; it is normal” — in a patient with AFib, loud habitual snoring is a red flag, not a normal variant. STOP-BANG is mandatory. ▸CPAP “sometimes, for a couple of hours” — the therapeutic effect is achieved with use ≥4 h/night, ≥70% of nights. Less than that has no effect on AFib recurrence. ▸Sleeping pills instead of diagnosis — they treat the symptom of sleep fragmentation, worsen OSA, and mask the diagnosis. ▸Alcohol before bed to fall asleep more easily — the most common way to worsen OSA. Ethanol relaxes pharyngeal musculature and prolongs apneas.
🌀
When to seek evaluation
▸AFib of unknown etiology or resistant to antiarrhythmics ▸Before catheter ablation for AFib — STOP-BANG is mandatory in all patients ▸Loud habitual snoring + daytime sleepiness + BMI >30 + hypertension ▸Witnessed breathing pauses during sleep ▸Refractory hypertension (requires ≥3 medications) ▸Morning headaches, impaired concentration, falling asleep while driving ▸Patients on hemodialysis, after stroke, or with heart failure — high probability of OSA ▸Family history of sudden cardiac death during sleep
I perform comprehensive cardio-somnology screening (STOP-BANG, home respiratory polygraphy when indicated, referral for polysomnography) and create a personalized OSA correction protocol in parallel with the rhythm strategy.
🌀
Conclusion
The link between obstructive sleep apnea and atrial fibrillation is not correlation; it is pathophysiology. OSA simultaneously creates both the trigger (pulmonary vein stretch) and the substrate (atrial fibrosis) for AFib. Without OSA correction, any rhythm-restoration strategy — antiarrhythmics or ablation — has only a temporary effect.
STOP-BANG is mandatory in all patients with newly diagnosed AFib. AHI ≥15 is an indication for CPAP before and after ablation. This is not cosmetic and not merely “lifestyle”; it changes the long-term outcome for decades.
Treat sleep, and the heart will be treated with it.
🌀
Sources
▸Gami AS, Hodge DO, Herges RM, et al. Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. *J Am Coll Cardiol* 2007;49:565–571. PMID 17719466 ▸Kanagala R, Murali NS, Friedman PA, et al. Obstructive sleep apnea and the recurrence of atrial fibrillation. *Circulation* 2003;107:2589–2594. PMID 12782568 ▸Linz D, McEvoy RD, Cowie MR, et al. Associations of obstructive sleep apnea with atrial fibrillation and continuous positive airway pressure treatment: a review. *JAMA Cardiol* 2018;3:532–540. PMID 29541763 ▸Patel D, Mohanty P, Di Biase L, et al. Safety and efficacy of pulmonary vein antral isolation in patients with obstructive sleep apnea: the impact of continuous positive airway pressure. *Circ Arrhythm Electrophysiol* 2010;3:445–451. PMID 20631252 ▸Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. *Anesthesiology* 2008;108:812–821. PMID 18431116
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
If I snore but do not feel daytime sleepiness, do I need evaluation? Yes, especially if AFib, hypertension, or BMI >30 is present. Up to 30% of patients with severe OSA do not report daytime sleepiness, particularly men and patients with long-term adaptation. STOP-BANG ≥3 points = evaluation, regardless of subjective symptoms.
Can I manage without CPAP? It depends on severity. With AHI 5–14 and minimal symptoms, positional therapy, MAD, and weight loss may be appropriate. With AHI ≥15 and AFib, CPAP is first-line therapy; alternatives (MAD, Inspire) are considered when CPAP is not tolerated. Weight loss of 10%+ can eliminate the indication for CPAP in some patients.
How quickly does CPAP affect AFib? The typical pattern is rhythm stabilization in patients with paroxysmal AFib after 4–12 weeks of regular use (≥4 h/night). Reduction in left atrial load on echocardiography occurs after 3–6 months. Reduction in post-ablation recurrence is assessed at 12 months.
I tolerate CPAP poorly. What should I do? First: change the mask (nasal mask, nasal pillows, full-face) with individualized fitting by a sleep specialist. Second: switch the mode to APAP with humidification. Third: consider alternatives — MAD for AHI <30, Inspire for selected indications. Fourth: aggressive weight reduction (bariatric surgery when BMI >35 with AFib and severe OSA).
Is ablation worthwhile if OSA is untreated? This decision is made jointly with an electrophysiologist. Technically, ablation is possible, but 5-year recurrence without CPAP is approximately 78%. In most cases, it is recommended to postpone ablation for 3–6 months of CPAP therapy to assess rhythm control; in some patients, AFib resolves with CPAP alone without a procedure.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 17719466. PMID 17719466
- PMID 20631252. PMID 20631252
- Kanagala R, Murali NS, Friedman PA, et al. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation 2003;107:2589–2594. PMID 12782568
- Linz D, McEvoy RD, Cowie MR, et al. Associations of obstructive sleep apnea with atrial fibrillation and continuous positive airway pressure treatment: a review. JAMA Cardiol 2018;3:532–540. PMID 29541763
- Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 2008;108:812–821. PMID 18431116