Introduction: the illusion of “normal” numbers
The standard lipid panel — total cholesterol, LDL-C, HDL-C, triglycerides — was developed in the 1960s for population screening. It is a tool of epidemiology, not personalized medicine. At the population level, it works: elevated LDL-C correlates with risk on average.
At the individual patient level, the standard panel misses 30–40% of cases of already developing atherosclerosis (Sniderman AD, Lancet 2003, PMID 12642066[1]). These people come in with “normal” numbers and leave with a reminder to “come back in a year.” Several years later comes the first myocardial infarction, which often becomes the first clinical manifestation of the disease.
Key point: modern markers — Lp(a), apoB, the apoB/apoA1 ratio, hsCRP, CAC-score, oxLDL — detect cardiovascular risk 10–15 years earlier than clinical events. This is the intervention window in which reversibility is supported by peer-reviewed data. It is precisely during this period that diet, physical activity, nutraceuticals, and, when necessary, pharmacotherapy have their greatest effect.
In this article, I review six functionally important markers: what they show, who should test them, how to interpret them, and what the next step should be.
🌀
Why the standard panel is insufficient
The standard lipid panel measures the mass of cholesterol carried in lipoproteins. But atherosclerosis is driven not by cholesterol mass, but by the number and quality of atherogenic particles that penetrate the subendothelial space.
A simple example: two patients have the same LDL cholesterol of 130 mg/dL. The first has large, “fluffy” LDL particles (pattern A). The second has small dense LDL (sdLDL, pattern B). The cholesterol mass is the same, but the second patient carries 2–3 times more particles, and these particles penetrate the endothelium, oxidize, and initiate atherogenesis far more readily. The standard panel will not distinguish between them.
Similarly, a patient with “normal” LDL-C and high Lp(a) of 80 mg/dL has the same risk as a patient with LDL-C of 200 mg/dL. Lp(a) is not visible on the standard test. It must be ordered separately — once in a lifetime.
🌀
Markers — the functionally important six
▸Lp(a) — the genetic “twin” of LDL. Structurally, it is an LDL particle + apolipoprotein(a) protein covalently bound to apoB-100. The Lp(a) level is 80–90% genetically determined and is not corrected by diet or physical activity. It is assessed once in a lifetime — the value does not change. Target <30 mg/dL (75 nmol/L). A high level is an independent risk factor for coronary artery disease, aortic stenosis, and stroke (Nordestgaard BG, Eur Heart J 2010, PMID 21118809[2]). ▸apoB — the number of atherogenic particles. Each LDL, VLDL, IDL, and Lp(a) particle carries exactly one molecule of apolipoprotein B-100 (or B-48 for chylomicrons). Measuring apoB directly counts the number of atherogenic particles circulating in the blood. It is more accurate than LDL cholesterol, especially in metabolic syndrome and insulin resistance, when LDL-C may be “normal” while the number of sdLDL particles is high. Target apoB <80 mg/dL (general prevention), <65 mg/dL (high risk). ▸ApoB/ApoA1 — the ratio of “bad/good” particles. ApoA1 is the main HDL protein. The apoB/apoA1 ratio is the best single predictor of myocardial infarction risk according to INTERHEART data (52 countries, 30,000 patients). Target <0.7 for women, <0.8 for men (Walldius G, Lancet 2001, PMID 11755611[3]). ▸hsCRP (high-sensitivity C-reactive protein) — a marker of vascular inflammation, not acute-phase bacterial inflammation. Target <1 mg/L. A level of 1–3 mg/L indicates moderate risk, >3 mg/L high risk. The JUPITER trial (Ridker PM, NEJM 2008, PMID 18997196[4]) demonstrated the predictive power of hsCRP even with normal LDL-C, as well as the benefit of statin therapy when LDL-C is <130 mg/dL + hsCRP >2 mg/L. ▸CAC-score (coronary artery calcium) — a structural marker. CT measurement of the volume of calcified plaques in the coronary arteries. Agatston scale: 0 — an event is unlikely within the next 10 years (Greenland P, JACC 2010, PMID 20428003[5]); 1–100 — mild atherosclerosis; 100–400 — moderate, statins indicated; >400 — severe, aggressive therapy. A single measurement at age 40–55 provides a fundamental understanding of individual risk. ▸oxLDL — oxidized LDL. The active substrate for macrophage transformation into foam cells. It is not included in the standard panel. It is available in commercial laboratories. It is a marker of an active atherogenic process, especially in antioxidant and omega-3 deficiency.
🌀
Drivers of elevated markers
Each marker has specific drivers. Understanding the cause determines the strategy:
•Lp(a) — genetics. It is not corrected by diet, physical activity, or standard statins. It is reduced by niacin (2 g/day, by 20–30%) and new agents (antisense oligonucleotide pelacarsen — phase III). With high Lp(a), the focus is aggressive control of the other markers. •apoB and sdLDL — insulin resistance, visceral obesity, a high-glycemic-index diet, omega-3 deficiency, genetics (FH). Corrected with a Mediterranean/DASH diet, resistance training, omega-3, bergamot, and statins when necessary. •hsCRP — visceral obesity, insulin resistance, gut dysbiosis, chronic infections (periodontitis, H. pylori), chronic stress, sleep deprivation, trans fats. Corrected by eliminating inflammatory triggers, omega-3, curcumin, and normalization of sleep and the microbiome. •CAC-score — reflects cumulative history. It rarely decreases (statins can stabilize plaques, while calcification may even increase on them — but qualitatively: “soft” plaques transform into stable “hard” plaques). It is used for risk stratification, not as a target for dynamic correction. •oxLDL — oxidative stress, antioxidant deficiency (vitamin C, E, selenium), low omega-3 index, smoking. Corrected with polyphenols, omega-3, smoking cessation, and a mitochondrial restoration protocol.
🌀
Who should test these markers (prioritization)
Not everyone needs all six markers at once. The strategy depends on age, history, and risk factors:
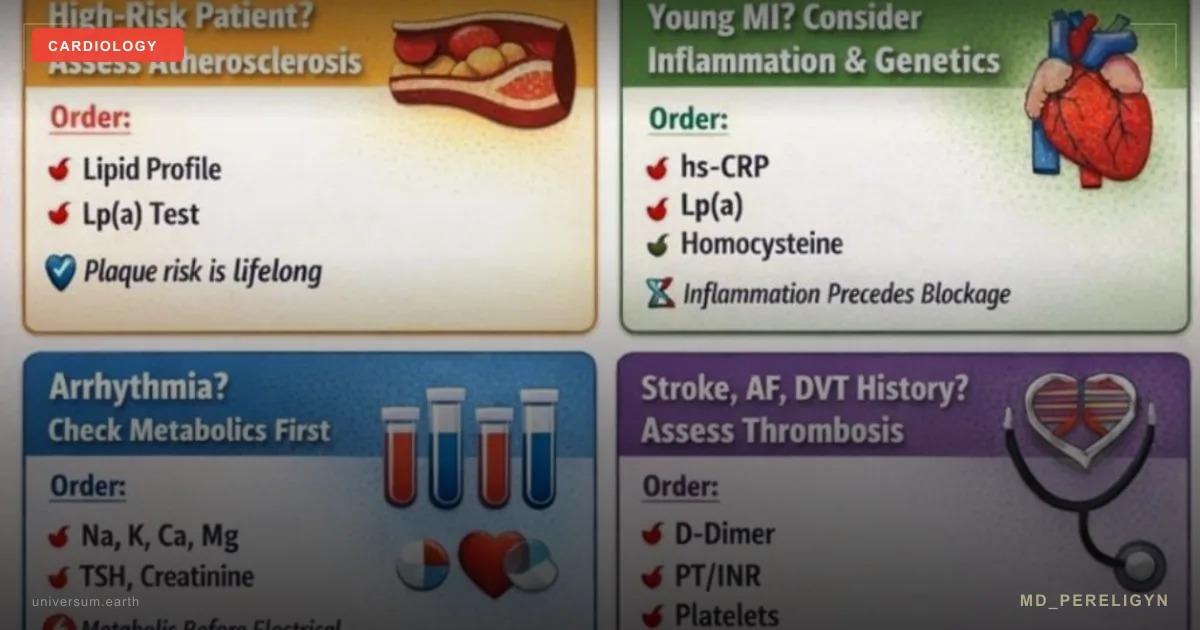
•Family history of coronary artery disease, myocardial infarction, or stroke in relatives before age 55 (men) or 65 (women) — Lp(a) is mandatory (at least once), as well as apoB, apoB/apoA1, and hsCRP. This is a critical group. •Age 40+ without symptoms — apoB, hsCRP, CAC-score (CT scan, dose 1 mSv). If CAC-score is zero, repeat after 5–10 years. •Metabolic syndrome, insulin resistance, prediabetes, type 2 diabetes — all six markers, plus HbA1c, fasting insulin, HOMA index, and small dense LDL (sdLDL). •“Normal” lipid panel + strong concern — Lp(a) (to exclude a genetic factor), hsCRP (to exclude subclinical inflammation). If both are normal, the risk is probably truly low. •Age 55+ without a CAC-score — it is reasonable to perform it once for baseline stratification.
🌀
Target values and interpretation
Summary table for practical interpretation:
▸Lp(a): optimal <30 mg/dL (75 nmol/L). Borderline 30–50 mg/dL. High >50 mg/dL (aggressively control the other markers). Very high >180 mg/dL (risk comparable to heterozygous familial hypercholesterolemia). ▸apoB: general prevention <80 mg/dL. Moderate risk <70 mg/dL. High risk <65 mg/dL. Very high risk (CAC>100, diabetes, history of coronary artery disease) <55 mg/dL. ▸apoB/apoA1: men <0.8, women <0.7. High risk >1.0 (men), >0.9 (women). ▸hsCRP: <1 mg/L — low risk. 1–3 mg/L — moderate. >3 mg/L — high. >10 mg/L — acute infection/inflammation; do not interpret as a vascular marker. ▸CAC-score: 0 — excellent. 1–100 — mild. 100–400 — moderate (statins indicated). >400 — severe (aggressive therapy, consider invasive diagnostics if symptomatic). ▸oxLDL: <60 U/L — low. >100 U/L — high risk. ▸Omega-3 index (as context) >8% protective, <4% — risk zone.
🌀
The next step — a holistic protocol
Obtaining tests is diagnosis. The next step is action. The principle of the md_pereligyn protocol: restoration of endothelial function and reduction of atherogenic burden at the particle level, not only cholesterol mass.
### 1. With high apoB and sdLDL
▸Mediterranean / DASH pattern — olive oil, fish 2 times per week, vegetables, nuts, legumes. Reduces apoB by 10–20% in 8–12 weeks. ▸Bergamot extract 500–1000 mg/day — reduces LDL-C and apoB through inhibition of HMG-CoA reductase (gentler than statins). ▸Soluble fiber (psyllium, oats) 10–25 g/day — binds bile acids and lowers LDL-C. ▸Resistance training 2–3 times/week — improves insulin sensitivity and reduces the proportion of sdLDL.
### 2. With high hsCRP
▸Omega-3 EPA+DHA 2 g/day (TOTOX <26) — a powerful anti-inflammatory effect. ▸Curcumin (with BioPerine) 500–1000 mg/day — NF-κB inhibition. ▸Polyphenols: pomegranate 250–500 mg, cocoa flavanols 500 mg, berries daily, green tea. ▸Vitamin D3 up to 60–80 ng/mL, doses of 4,000–10,000 IU/day individually + K2 (MK-7) 100–200 mcg. ▸Audit of inflammation sources: periodontitis, H. pylori, gut dysbiosis, hidden food intolerances.
### 3. With high Lp(a)
▸Aggressive control of modifiable markers: apoB <55 mg/dL, hsCRP <1 mg/L, omega-3 index >8%. ▸Niacin 1000–2000 mg/day — reduces Lp(a) by 20–30% (weigh adverse effects, discuss with a physician). ▸Aspirin 81 mg/day — consider with Lp(a) >50 mg/dL and other risk factors (USPSTF 2022 recommendations, individualized). ▸Regular CAC monitoring — every 3–5 years.
### 4. With high oxLDL
▸Vitamin C 500–1000 mg/day + vitamin E (tocopherols + tocotrienols, mixed forms) 200–400 IU. ▸Selenium 100–200 mcg/day — a cofactor of glutathione peroxidase. ▸Polyphenols (see above) — powerful antioxidants in the subendothelial space. ▸Smoking cessation — priority No. 1.
🌀
What does NOT work (and why)
▸Using only the standard lipid panel to assess individual risk — misses 30–40% of atherosclerosis cases. ▸Ignoring Lp(a) in young patients with a family history — a missed opportunity for stratification decades earlier. ▸Lowering LDL-C without assessing apoB — sometimes LDL-C falls while apoB and the number of sdLDL particles remain high (a mismatch between mass and particle number). ▸hsCRP during an acute infection — not representative. Test in a stable condition at least 2 weeks after infection. ▸Repeating CAC scanning more often than once every 3–5 years — radiation exposure is not justified. CAC changes slowly. ▸“My CAC is good = I can eat anything” — a zero CAC today does not guarantee a zero CAC in 10 years, especially with poor habits.
🌀
When to seek consultation
▸Family history of coronary artery disease before age 60 — for baseline Lp(a) assessment and risk stratification ▸Age 40+ without CAC-score assessment ▸“Normal” lipid panel + fatigue, poor recovery, high blood pressure ▸Metabolic syndrome, insulin resistance, prediabetes ▸A desire to undergo extended cardiometabolic screening with interpretation of all markers and development of a personalized protocol
I perform full extended screening (Lp(a), apoB, apoB/apoA1, hsCRP, sdLDL, oxLDL, omega-3 index, and, when indicated, CAC-score) with detailed interpretation and development of a holistic protocol.
🌀
Conclusion
The standard lipid panel is a tool of population epidemiology, not personalized medicine. It misses 30–40% of patients with already developing atherosclerosis. Modern markers — Lp(a), apoB, apoB/apoA1, hsCRP, CAC-score, oxLDL — detect risk 10–15 years before clinical events.
Main practical point: Lp(a) — once in a lifetime for everyone with a family history of coronary artery disease. apoB and hsCRP — every 1–2 years for everyone 40+. CAC-score — once at age 40–55 for baseline stratification. This is the intervention window in which atherosclerosis is reversible. A number without context is an illusion of health.
Deeper analysis means earlier prevention.
🌀
Sources
▸Nordestgaard BG, Chapman MJ, Ray K, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. *Eur Heart J* 2010;31:2844–2853. PMID 21118809 ▸Sniderman AD, Furberg CD, Keech A, et al. Apolipoproteins versus lipids as indices of coronary risk and as targets for statin treatment. *Lancet* 2003;361:777–780. PMID 12642066 ▸Ridker PM, Cushman M, Stampfer MJ, et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. *N Engl J Med* 1997;336:973–979. PMID 9077376 ▸Greenland P, Bonow RO, Brundage BH, et al. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring. *J Am Coll Cardiol* 2010;55:e185–e210. PMID 20428003 ▸Walldius G, Jungner I, Holme I, et al. High apolipoprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. *Lancet* 2001;358:2026–2033. PMID 11755611 ▸Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein (JUPITER). *N Engl J Med* 2008;359:2195–2207. PMID 18997196
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
If Lp(a) is measured once in a lifetime, when should I test it? Optimally at age 18–25 for baseline stratification, especially with a family history of coronary artery disease. If you have not tested it before, test it now, at any age. The level remains practically unchanged throughout life (variation <10–15%).
Why do I need apoB if LDL-C exists? apoB directly counts the number of atherogenic particles. LDL cholesterol is the mass of cholesterol in those particles. In metabolic syndrome and sdLDL, there are many particles, but they are small — the cholesterol mass may be “normal,” while the particle number is high. apoB predicts risk more accurately.
Is CAC scanning safe? What is the radiation dose? The dose is about 1 mSv — comparable to background radiation over 4 months or one transatlantic flight. It is safe for repeat use every 3–5 years. Its informational value greatly outweighs the risks.
Can Lp(a) be lowered by natural methods? Only to a very limited extent. Lp(a) is 80–90% genetically determined. Niacin (1–2 g/day) reduces it by 20–30%, but has adverse effects (flushing, increased glucose). New drugs (pelacarsen, olpasiran) show reductions of 80–90% in phase III. For most people, the strategy is aggressive control of modifiable factors.
What should I do if all markers are normal, but my family history is burdened? Repeat the extended panel every 2 years starting at age 35–40. Control modifiable factors (nutrition, movement, sleep, stress, omega-3 index). If any concerning marker appears, move to more frequent monitoring and active intervention. Family history is not a reason for anxiety, but for systematic prevention.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 12642066. PMID 12642066
- PMID 21118809. PMID 21118809
- PMID 11755611. PMID 11755611
- PMID 18997196. PMID 18997196
- PMID 20428003. PMID 20428003
- Ridker PM, Cushman M, Stampfer MJ, et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997;336:973–979. PMID 9077376