Introduction: Silence Is Not Safety
“I have no pain” is the most dangerous phrase in cardiology. Up to one third of all myocardial ischemia episodes occur without classic anginal pain: no pressing retrosternal burning, no radiation to the left arm, no characteristic discomfort. This is painless, or silent myocardial ischemia (SMI).
Silence does not mean lower risk. The prognosis in silent ischemia is often worse than in typical angina because the patient does not seek help, and the clinician sees no changes on a standard resting ECG. The diagnosis is made retrospectively: after myocardial infarction, after sudden cardiac death, or after the first coronary angiography showing “newly diagnosed” three-vessel disease.
Key principle of the md_pereligyn protocol: pain is not a prerequisite for ischemia. In a patient from a risk group, an atypical signal requires instrumental assessment, not watchful waiting.
This article explains why a standard ECG systematically misses painless ischemia, who is at highest risk, and which early diagnostic protocol actually works.
🌀
Epidemiology: The Scale of a Hidden Problem
According to the Multi-Ethnic Study of Atherosclerosis (MESA) and the Framingham Heart Study, among patients with verified coronary artery disease, 20–40% of ischemic episodes are completely asymptomatic (Cohn PF, Circulation 2003, PMID 12796124[1]). In patients with type 2 diabetes, this figure reaches 60% (Wackers FJ, Diabetes Care 2004, PMID 15047686[2]).
Painless ischemia is not rare and not anecdotal; it is the dominant clinical form of coronary artery disease in certain patient groups. In women, people with diabetes, older adults, and post-infarction patients, classic angina is the exception rather than the rule.
At the same time, the risk of myocardial infarction and cardiovascular death in patients with silent ischemia is comparable to, or even higher than, that in patients with typical painful ischemia (Deedwania PC, Circulation 2007, PMID 17088460[3]).
🌀
Mechanism: Why Pain “Does Not Arrive”
Chest pain during ischemia is a signal that passes through a chain: ischemic cardiomyocyte → afferent sympathetic fibers → dorsal horns of the spinal cord at T1–T5 → thalamus → cortex. Any disruption in this chain masks the symptom.
▸Vegetative (autonomic) neuropathy is the main mechanism in people with diabetes and patients with CKD. Hyperglycemia damages small myelinated fibers; the nociceptive signal is lost on its way to the CNS. ▸Altered myocardial innervation after infarction: scar tissue and denervated segments do not transmit pain signals. ▸High pain threshold in older adults: reduced nociceptor density and altered central signal processing. ▸Sex differences in cortical pain processing: women more often present atypically, with dyspnea, fatigue, jaw discomfort, or epigastric discomfort instead of classic retrosternal pain (Mehta LS, Circulation 2016, PMID 26831993[4]). ▸Short ischemic episodes: shorter than 5 minutes, insufficient to trigger a pain response but already capable of causing electrical instability.
In other words: ischemia is present, metabolic injury is occurring, the ST segment is already depressed on Holter monitoring, but the cortex does not receive the “pain” signal. The heart signals differently: through dyspnea, fatigue, nocturnal heaviness, and declining exercise tolerance.
🌀
6 Atypical Signals: What to Look For
If classic angina is “retrosternal pressure with exertion that resolves at rest,” the atypical signals of silent ischemia look different:
▸Sudden dyspnea during usual exertion is the most common atypical equivalent. Climbing the same stairs as a month ago now causes shortness of breath. ▸Chronic fatigue unrelated to sleep: ischemic myocardium reduces cardiac output, and skeletal muscles receive less oxygen. ▸Nocturnal awakenings with chest heaviness: nocturnal decubitus angina, often misclassified as “panic attacks” or GERD. ▸Unexplained cold sweating with minimal exertion: sympathetic activation in response to ischemia. ▸Discomfort in the jaw, interscapular back, or epigastrium during movement: radiation through alternative pathways. ▸Decline in exercise tolerance over weeks or months: nonspecific, but often the only signal in older adults.
None of these symptoms is diagnostic on its own. But a combination of several atypical signals in a patient from a risk group is an indication for instrumental assessment, not for prescribing antidepressants or antacids.
🌀
5 Risk Groups: Who Misses Classic Angina
The atypical presentation of painless ischemia does not occur in everyone, but in certain groups it becomes the dominant form.
•Women 50+: atypical presentation by default. Microvascular disease, coronary artery spasm, and INOCA (ischemia with non-obstructive coronary arteries) all produce less “classic” pain. Hospitalization occurs, on average, 6 hours later than in men. •Diabetes for 5+ years: autonomic neuropathy. The longer the duration of diabetes and the poorer the compensation, the higher the risk of missing ischemia. In patients with HbA1c >8% for more than 5 years, every second ischemic episode is painless. •Post-infarction patients: altered myocardial innervation after necrosis. The paradox is that after a first infarction, the risk of recurrent events increases while the ability to feel ischemia decreases. •Chronic kidney disease (CKD): coronary artery calcification progresses without symptoms but is visually detectable on CT. •Older adults 75+: altered pain threshold and masking of symptoms by chronic comorbidities.
If you belong to at least one of these groups, a standard resting ECG at an annual check-up is not sufficient. Targeted instrumental assessment is needed.
🌀
Markers and Diagnostics: What Actually Shows Ischemia
A standard resting ECG is a low-sensitivity tool for detecting painless ischemia. Episodes are short, transient, and may be absent at the time of recording. What actually works:
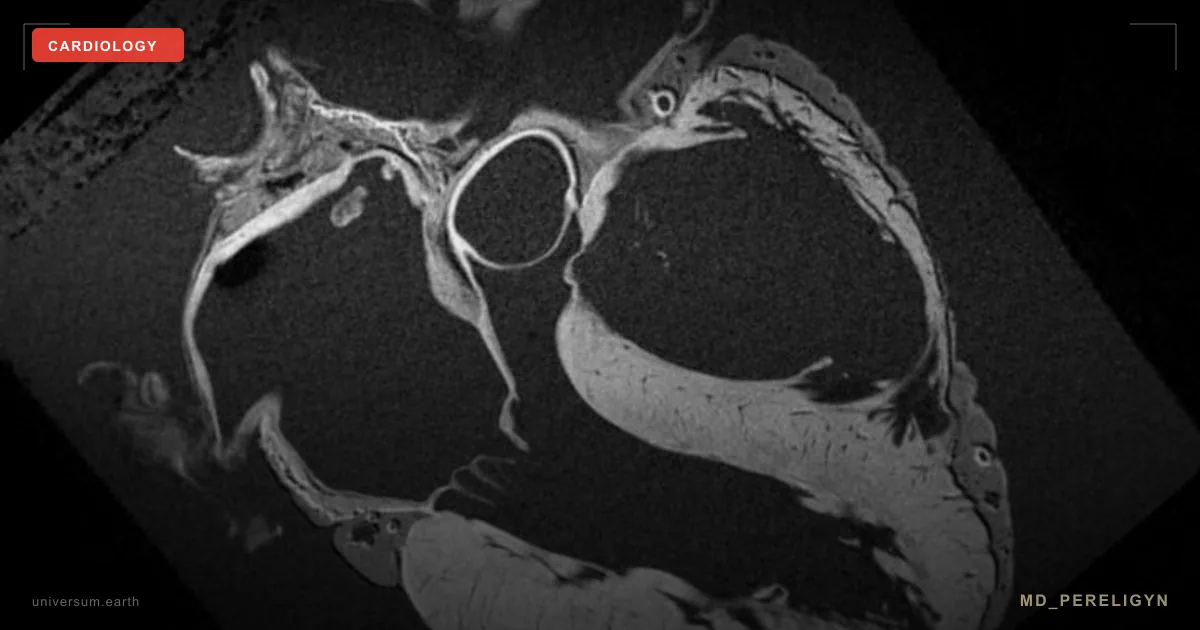
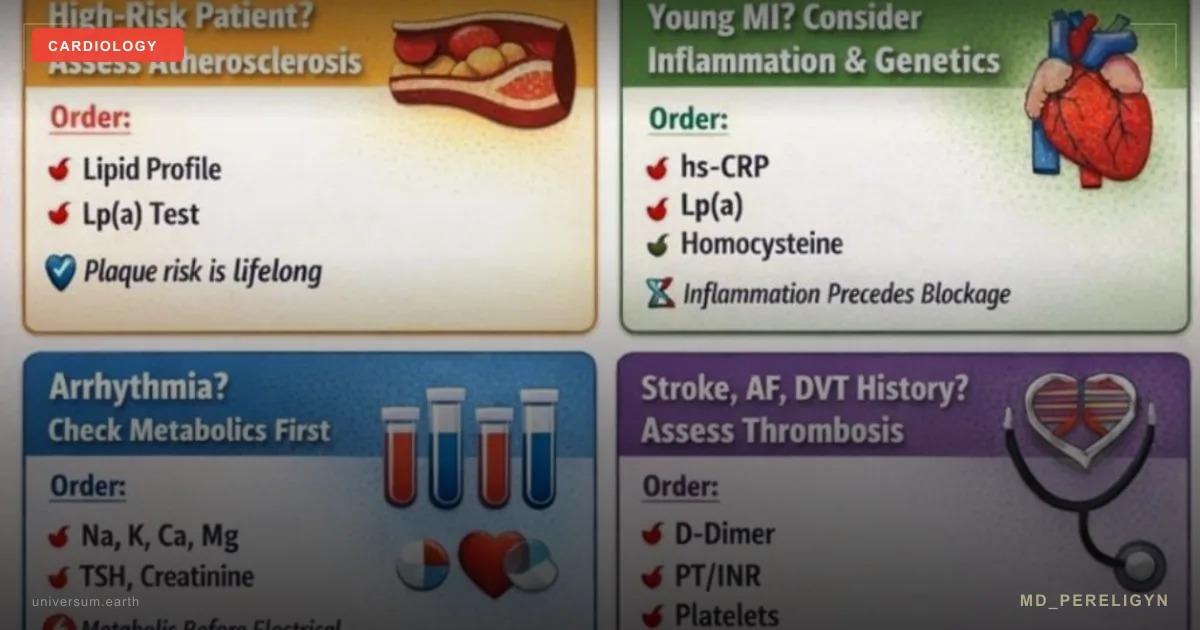
▸CAC-score (coronary artery calcium): non-contrast computed tomography of the coronary arteries with calcification assessment. Normal is 0, risk zone >100, high risk >400. CAC >0 in a patient younger than 50 years is an indication for expanded evaluation (Greenland P, JACC 2010, PMID 20428003[5]). ▸Stress echocardiography: exercise or pharmacologic stress testing with ultrasound assessment of regional contractility. Sensitivity is ~80%, specificity ~85%. No radiation exposure and more accessible than CT coronary angiography. ▸Cardiac MRI (CMR) with pharmacologic stress: the gold standard for perfusion assessment. Especially useful in INOCA and microvascular disease. ▸Holter ECG for 24–72 hours: monitoring during usual daily life, detecting painless episodes of ST depression. ST depression ≥1 mm lasting ≥1 minute is considered ischemic. ▸Biochemical markers: lipids (including one-time Lp(a), sdLDL, apoB), hsCRP (target <1 mg/L), HbA1c (target <5.7%), NT-proBNP (increases with myocardial overload), homocysteine. ▸Exercise ECG (treadmill test): ST depression ≥1 mm during exertion. Sensitivity is lower in women and in single-vessel disease. ▸CT coronary angiography (CCTA) with assessment of stenosis and plaque characteristics (lipid-rich, fibrous, calcified, low-attenuation).
Target strategy: once per year in the presence of 2+ risk factors: reassessment with CAC-score or stress echocardiography. In patients with CAC >100: annual treatment review. In patients with diabetes for 5+ years: Holter monitoring once every 1–2 years.
🌀
Holistic Protocol: Early Diagnosis and Risk Reduction
The goal is to detect ischemia at a stage when functional reversibility is still possible. The principle of the md_pereligyn protocol is screening by risk group, not by symptoms. Waiting for pain means missing the intervention window.
### 1. Screening by Risk Group
▸CAC-score: once at age 40–50 years for all men and women with risk factors (family history, diabetes, hypertension, smoking, dyslipidemia). Repeat after 5 years if CAC = 0; annually if CAC >100. ▸Holter ECG for 48–72 h: for patients with diabetes for 5+ years, post-infarction status, CKD, or CHF. ▸Stress echocardiography: when CAD is suspected in women; more sensitive than treadmill ECG. ▸Expanded biochemistry 1–2 times/year: one-time Lp(a), hsCRP, HbA1c, omega-3 index, sdLDL, apoB/apoA1.
### 2. Reducing Global Vascular Risk
▸Blood pressure control: target <130/80 in high-risk patients (SPRINT, NEJM 2015, PMID 26551272[6]). Independent home monitoring in the morning and evening. ▸LDL-C: target <70 mg/dL (1.8 mmol/L) at high risk; <55 mg/dL (1.4 mmol/L) at very high risk (after infarction, diabetes with target-organ damage). ▸HbA1c: target <6.5% in younger patients with diabetes, <7% in older adults. ▸Waist circumference: <94 cm in men, <80 cm in women. Visceral fat is an independent predictor of vascular events.
### 3. Supporting the Endothelium and Coronary Reserve
A detailed protocol for restoring endothelial function is a separate article. Key elements:
▸Omega-3 (EPA+DHA) 2 g/day: target omega-3 index >8%. At high risk, target EPA 4 g/day (REDUCE-IT). ▸Magnesium (glycinate / taurate) 400 mg: eNOS cofactor, antiarrhythmic effect. ▸Vitamin D3 4000–6000 IU + K2 (MK-7) 100–200 μg: target 25(OH)D 60–80 ng/mL. ▸Polyphenols: pomegranate (extract) 250–500 mg, cocoa (flavanols) 500 mg, resveratrol 250 mg. Support BH4 regeneration and NO bioavailability. ▸L-citrulline 3 g/day: increases plasma arginine and improves FMD.
### 4. Antithrombotic Strategy: Individualized
▸Aspirin 75–100 mg: only in confirmed CAD, after acute myocardial infarction, with CAC >300, or based on individualized risk-benefit assessment. Current recommendations (USPSTF 2022) do not support aspirin for primary prevention in patients without clear risk because bleeding outweighs benefit. ▸Statins: for LDL-C >100 mg/dL and high risk, CAC >100, or familial hypercholesterolemia. Not “for everyone after 50,” but based on individualized assessment.
### 5. Lifestyle and Rehabilitation
▸Aerobic activity 30+ minutes/day: walking, swimming, cycling. Activates laminar shear stress and eNOS. ▸Resistance training 2–3 times/week: supports muscle mass and insulin sensitivity. ▸Sleep 7–9 hours: endothelial repair window and reduction of sympathetic tone. ▸Stress management: breathing practices, meditation, digital hygiene. Cortisol is a direct driver of endothelial dysfunction. ▸Smoking cessation: the effect on coronary risk is visible after 12 months.
🌀
What Does NOT Work and Why
▸Standard resting ECG as the only screening tool: misses 70–80% of painless episodes. Use only in combination with Holter monitoring, CAC, and stress testing. ▸“I have no pain, so everything is fine”: in a person with diabetes for 5+ years, this statement is statistically false. Absence of pain does not mean absence of ischemia. ▸Prescribing nitrates “for discomfort” without diagnostic verification: masks symptoms and delays real diagnosis. ▸Ignoring atypical signals in women: a frequent cause of late diagnosis and worse prognosis. Women with dyspnea and fatigue receive cardiology consultation, on average, 1–2 years later than men with typical pain. ▸Prescribing antidepressants for “panic attacks” in patients from risk groups without cardiologic assessment: possible nocturnal decubitus angina is missed. ▸Preventive aspirin “for everyone after 50”: contemporary data (ASPREE, NEJM 2018, PMID 30221596[7]) showed no benefit and an increased bleeding risk in older adults without clear risk factors.
🌀
When to Seek Assessment
▸Family history of CAD, myocardial infarction, or sudden death before age 60 ▸Type 2 diabetes with duration 5+ years ▸Poorly controlled arterial hypertension (BP >140/90 on therapy) ▸Metabolic syndrome, prediabetes, visceral obesity ▸Chronic kidney disease (eGFR <60) ▸Post-infarction status, prior MI, or a previous “false alarm” cardiology presentation ▸Atypical signals: dyspnea, fatigue, nocturnal chest heaviness, decline in exercise tolerance over the past 3–6 months ▸Women 50+ with any cardiovascular risk factors
I provide comprehensive screening with CAC-score, an expanded lipid profile (sdLDL, Lp(a), apoB), Holter ECG when indicated, and a personalized risk-reduction protocol.
🌀
Conclusion
Silent myocardial ischemia is not a rare disorder but a dominant clinical form of coronary artery disease in women, people with diabetes, post-infarction patients, and older adults. A standard resting ECG systematically misses it, and waiting for classic textbook pain is a strategy with a worse prognosis than active screening.
The principle of the md_pereligyn protocol is screening by risk group, not by symptoms. CAC-score, Holter monitoring, stress echocardiography, and expanded biochemistry are tools that detect ischemia years before myocardial infarction. At this stage, reversibility is evidence-based: correction of blood pressure, LDL-C, glycemia, omega-3 index, and endothelial function meaningfully reduces cardiovascular events.
Pain is not a prerequisite for ischemia. Silence is not safety. Detecting it earlier means treating the vessel, not its complications.
🌀
Sources
▸Cohn PF, Fox KM, Daly C. Silent myocardial ischemia. *Circulation* 2003;108:1263–1277. PMID 12796124 ▸Wackers FJ, Young LH, Inzucchi SE, et al. Detection of silent myocardial ischemia in asymptomatic diabetic subjects: the DIAD study. *Diabetes Care* 2004;27:1954–1961. PMID 15047686 ▸Mehta LS, Beckie TM, DeVon HA, et al. Acute myocardial infarction in women: a scientific statement from the American Heart Association. *Circulation* 2016;133:916–947. PMID 26831993 ▸Greenland P, Bonow RO, Brundage BH, et al. ACCF/AHA 2010 guidelines on coronary artery calcium scoring. *J Am Coll Cardiol* 2010;56:e50–e103. PMID 20428003 ▸Knuuti J, Wijns W, Saraste A, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. *Eur Heart J* 2020;41:407–477. PMID 31504439 ▸Deedwania PC, Carbajal EV. Silent ischemia during daily life: clinical and prognostic significance. *Circulation* 2007;116:2802–2812. PMID 17088460 ▸Ridker PM, Danielson E, Fonseca FA, et al. JUPITER trial: rosuvastatin to prevent vascular events in men and women with elevated CRP. *N Engl J Med* 2008;359:2195–2207. PMID 18997196 ▸SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. *N Engl J Med* 2015;373:2103–2116. PMID 26551272 ▸McNeil JJ, Wolfe R, Woods RL, et al. ASPREE: aspirin in older persons. *N Engl J Med* 2018;379:1509–1518. PMID 30221596
Related articles: Endothelium: The Foundation of Vascular Health, Cholesterol Without Statins.
🌀
FAQ
If I have no chest pain, do I need cardiac screening? If you belong to at least one risk group (diabetes for 5+ years, woman 50+ with hypertension or dyslipidemia, post-infarction status, CKD, family history of CAD before age 60), then yes, absolutely. Painless ischemia is a statistically common form in these groups. CAC-score and Holter ECG can detect it years before clinical presentation.
Is a standard resting ECG sufficient to exclude CAD? No. A standard resting ECG misses up to 70–80% of painless ischemic episodes. Diagnosis requires stress tests (stress echocardiography, treadmill testing), Holter monitoring, CAC-score, and, when necessary, CT coronary angiography or CMR with perfusion.
What is CAC-score and who needs it? CAC-score (coronary artery calcium) is non-contrast computed tomography of the coronary arteries that quantifies calcification in Agatston units. Normal is 0, risk zone >100, high risk >400. It is indicated for men and women aged 40–50+ with risk factors. It is a one-time test with low radiation exposure (~1 mSv), and the result changes management in 30–40% of cases.
Can myocardial function be restored if silent ischemia is detected? Yes, partially, if it is detected before infarction. Correction of blood pressure, LDL-C, glycemia, omega-3 index, restoration of endothelial function, and lifestyle optimization slow atherosclerosis progression. Rehabilitation after ischemic episodes improves FMD and coronary reserve.
Should I take aspirin “for prevention” if I have risk factors? No, not “for everyone after 50.” Current recommendations (USPSTF 2022, ASPREE) do not support aspirin for primary prevention in patients without confirmed CAD because bleeding risk exceeds benefit. Aspirin is prescribed individually: in confirmed CAD, after acute myocardial infarction, with CAC >300, and after assessing bleeding risk.
*This article is for informational purposes and does not replace medical consultation. Before starting any nutraceuticals, changing medication therapy, or undergoing diagnostic procedures, discuss the plan with your treating physician.*
References
- PMID 12796124. PMID 12796124
- PMID 15047686. PMID 15047686
- PMID 17088460. PMID 17088460
- PMID 26831993. PMID 26831993
- PMID 20428003. PMID 20428003
- PMID 26551272. PMID 26551272
- PMID 30221596. PMID 30221596
- Knuuti J, Wijns W, Saraste A, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41:407–477. PMID 31504439
- Ridker PM, Danielson E, Fonseca FA, et al. JUPITER trial: rosuvastatin to prevent vascular events in men and women with elevated CRP. N Engl J Med 2008;359:2195–2207. PMID 18997196