Introduction: the factor missing from the standard lipid panel
When a patient has a myocardial infarction at age 45 despite “normal” LDL, cardiologists often have no obvious explanation. Cholesterol is not to blame, blood pressure is normal, there is no diabetes, and the patient does not smoke. Where is the source? In half of cases, it is where the standard test simply does not look. This is Lp(a) (lipoprotein(a), lipoprotein little a).
Lp(a) is an LDL particle with an additional apoprotein, apo(a), genetically encoded by the LPA gene on chromosome 6. This addition turns ordinary LDL into a particularly atherogenic and prothrombotic particle. The level is 70–90% heritable and changes very little throughout life (Kronenberg F, Eur Heart J 2022, PMID 36302098[1]). Diet, exercise, and statins do almost nothing.
Key idea of the md_pereligyn protocol: about 20% of the population has a clinically significant elevation of Lp(a) (>50 mg/dL or >125 nmol/L). They inherited their risk of myocardial infarction and aortic stenosis, and they do not even know it because Lp(a) is not part of a standard checkup.
This omission can cost lives. Lp(a) is the only major risk factor that is measured with one test, once in a lifetime, and immediately provides a reference point for decades ahead.
🌀
Why Lp(a) is more dangerous than ordinary LDL
Lp(a) combines three pathogenic properties in one particle:
▸LDL-like atherogenicity — apo(a) sits on an apoB-100 base; the particle penetrates the subendothelial space, becomes oxidized, and promotes foam cells and fibroatheroma. ▸Prothrombotic effect — apo(a) is homologous to plasminogen. It competes with plasminogen for receptors and reduces fibrinolysis. Microthrombi dissolve less effectively, turning a stable plaque into an unstable one. ▸Procalcific effect — Lp(a) carries oxidized phospholipids (oxPL), which activate osteogenic transformation of aortic valve interstitial cells. This is a leading mechanism of calcific aortic stenosis in young and middle-aged adults.
High Lp(a) increases myocardial infarction risk 2–3-fold, stroke risk 1.5–2-fold, and aortic stenosis risk 2–3-fold independently of LDL and ApoB (Tsimikas S, J Am Coll Cardiol 2017, PMID 28057251[2]).
🌀
One test for life
The unique feature of Lp(a) is stability. Its level is determined by genetics and barely responds to lifestyle. Therefore:
▸Test once — usually after age 18; in children with a strong family history, testing can be done from age 5–10. ▸Repeat testing is not needed, except in rare situations: severe systemic diseases, nephrotic syndrome, hypothyroidism (which can temporarily raise Lp(a)), and pregnancy (physiologic increase). ▸Units of measurement: mg/dL and nmol/L are different scales and cannot be converted linearly. Modern laboratories use nmol/L as the standard. Target <75 nmol/L (≈ <30 mg/dL), borderline 75–125 nmol/L, high >125 nmol/L (>50 mg/dL). ▸Family strategy: if one parent has Lp(a) > 50 mg/dL, children and siblings should be tested.
🌀
Drivers and categories of Lp(a)
Lp(a) is not something that “appears under stress,” unlike many markers. It is a lifelong background level. But interpretation depends on the category:
•Low, <30 mg/dL (<75 nmol/L) — no increased genetic risk. This is about 50% of the population. •Intermediate, 30–50 mg/dL (75–125 nmol/L) — mild elevation, requiring attention. It does not independently mandate therapy, but it strengthens the need for aggressive control of other factors. •High, 50–180 mg/dL (125–450 nmol/L) — clinically significant elevation, ~20% of the population. Active strategy to reduce total atherogenic burden. •Very high, >180 mg/dL (>450 nmol/L) — risk equivalent to familial hypercholesterolemia. ~1% of the population. Family screening, discussion of PCSK9 inhibitors and, in the near future, RNA agents are indicated.
🌀
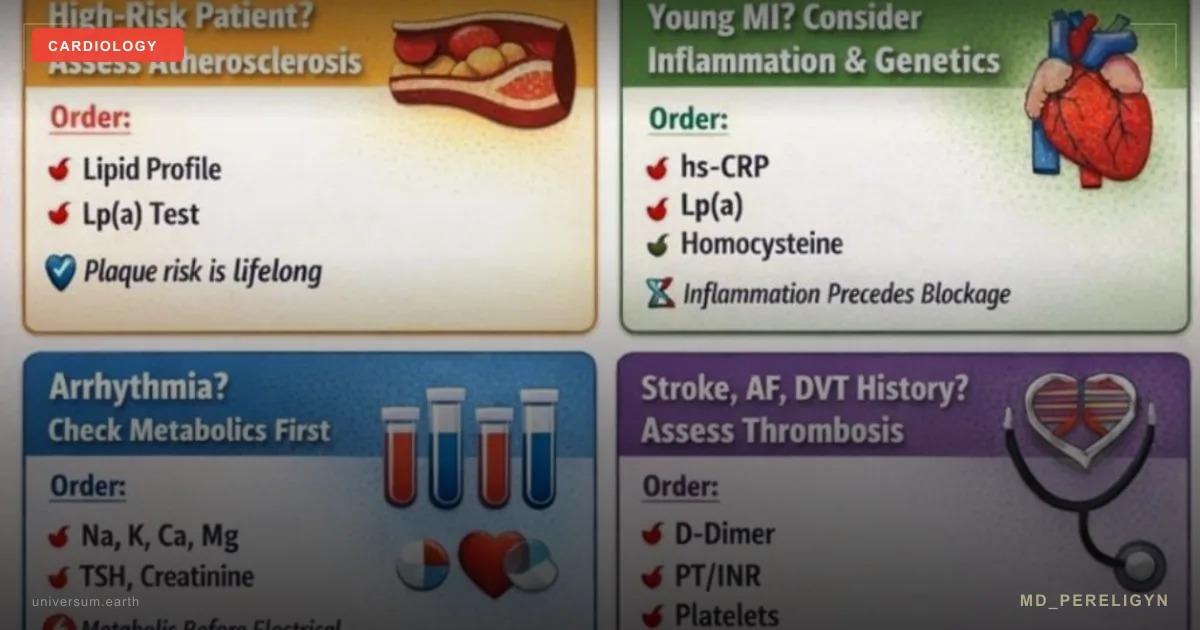
Markers to test together with Lp(a)
Lp(a) itself is a number. To interpret it correctly and make decisions, it is logical to include the following in one panel:
▸ApoB — the main marker of the number of atherogenic particles. Target <80 mg/dL (general population), <65 mg/dL (high risk, including Lp(a) > 50). ▸Advanced lipid panel — total cholesterol, LDL, HDL, triglycerides, sdLDL, oxLDL. ▸hsCRP — marker of vascular inflammation. Target <1 mg/L. ▸HbA1c, fasting insulin, glucose — metabolic background. ▸Homocysteine — cofactor of endothelial injury. ▸Omega-3 index — % EPA+DHA in erythrocytes. Target >8%. ▸Vitamin D 25(OH) — target 50–80 ng/mL. ▸CAC score — in patients 40+ to understand how much the genetic Lp(a) risk has already manifested as plaque.
🌀
Holistic protocol for high Lp(a)
The main strategic idea: for now, Lp(a) itself is almost impossible to reduce radically. Therefore the approach is to reduce the total atherogenic burden so aggressively that Lp(a) no longer finds a vulnerable vessel.
### 1. ApoB and LDL control
▸ApoB target <65 mg/dL when Lp(a) > 50 mg/dL (instead of the usual target <80 mg/dL). ▸Statin at an effective dose — rosuvastatin 10–20 mg or atorvastatin 20–40 mg. Note: a statin may slightly raise Lp(a) by 5–10%, but the reduction in overall atherogenicity outweighs this effect. ▸Ezetimibe 10 mg is added if the ApoB / LDL target is not reached. ▸PCSK9 inhibitors (alirocumab, evolocumab) reduce Lp(a) by 25–30% and ApoB by 50–60%. They are indicated in very high Lp(a) with insufficient response to statin + ezetimibe.
### 2. Blood pressure and glycemia
▸BP target <120/80 mm Hg in high Lp(a). Any blood pressure elevation increases wall stress and attacks vulnerable sites where Lp(a) has already deposited. ▸HbA1c <5.7%, fasting insulin <8 μIU/mL, HOMA-IR <1.5 — hyperglycemia and insulin resistance accelerate atherogenesis synergistically with Lp(a).
### 3. Endothelial protection
▸L-arginine 3–6 g/day or citrulline 3 g/day — substrate for NO synthase, supporting vasodilation. ▸Polyphenols: pomegranate (250–500 mg extract), cocoa (flavanols 500 mg), resveratrol (250–500 mg), quercetin (500 mg), EGCG (400 mg). ▸CoQ10 100–200 mg (especially on a statin), L-carnitine 1–2 g/day. ▸Magnesium (glycinate / taurate) 400 mg, vitamin K2 (MK-7) 100–200 μg + vitamin D3 4 000–8 000 IU.
### 4. Omega-3 — high dose
▸EPA+DHA 2–4 g/day — triglyceride reduction, anti-inflammatory action, plaque stabilization. ▸Icosapent ethyl (Vascepa) 4 g/day when available — REDUCE-IT data showed event reduction in high-risk patients. ▸Omega-3 index monitoring every 4–6 months, target >8%.
### 5. Lp(a)-specific options
▸Apheresis (plasmapheresis) — the only current method of substantially lowering Lp(a) (by 60–80% per session). It is indicated in severe Lp(a) with progressive atherosclerosis and is available in specialized cardiac centers in Europe and the United States. ▸RNA agents (pelacarsen, olpasiran, lepodisiran) — phase 3 clinical trials, with event data expected in 2026–2027. Lp(a) reduction by 80–95%. ▸Niacin — an outdated option; it lowers Lp(a) by 20–30%, but trials did not show event reduction and it has adverse effects. It is not recommended in modern protocols.
### 6. Aspirin
▸Aspirin 75–100 mg/day — discussed individually when Lp(a) > 50 mg/dL, especially in patients with additional risk factors and low bleeding risk. Apo(a) inhibits fibrinolysis; aspirin compensates for part of the prothrombotic effect.
### 7. Lifestyle
▸Complete smoking cessation — an absolute priority. Smoking and high Lp(a) synergistically increase risk. ▸Mediterranean / DASH diet, restriction of trans fats and omega-6. ▸Aerobic activity 150+ min/week + strength training 2–3 times/week — endothelial support. ▸Sleep 7–9 hours, stress control. ▸Annual checkup: ApoB, hsCRP, HbA1c, omega-3 index, ambulatory BP monitoring if needed.
🌀
What does NOT work
▸Statins as a way to lower Lp(a) — they lower LDL but do not lower Lp(a) (they may even raise it slightly). In Lp(a), statins are needed not to reduce Lp(a), but to reduce the total atherogenic burden. ▸Diet and exercise as an isolated strategy — they do not correct Lp(a). They are useful for everything else, but they do not move the Lp(a) number. ▸“Natural” remedies promising to lower Lp(a) — no randomized data. Do not waste money. ▸Niacin monotherapy — did not show event reduction and has adverse effects (flushing, hyperglycemia, hepatotoxicity). ▸Ignoring Lp(a) when cholesterol is “normal” — the main mistake of standard cardiology. Normal LDL with Lp(a) > 100 mg/dL is not “low risk”; it is missed risk. ▸Repeated Lp(a) measurement — except for exclusions (nephrotic syndrome, hypothyroidism, pregnancy, severe systemic disease). The level changes very little.
🌀
When to seek care
▸Family history of coronary artery disease / myocardial infarction / stroke before age 60 ▸Personal history of early myocardial infarction or ischemic stroke with “normal” LDL ▸Calcific aortic stenosis in young or middle age ▸ApoB > 100 mg/dL with borderline or normal LDL ▸Familial hypercholesterolemia (for deeper stratification) ▸Desire to assess genetic vascular risk once in a lifetime ▸Children and siblings of patients with known Lp(a) > 50 mg/dL
I perform full vascular stratification (Lp(a), ApoB, advanced lipid panel, hsCRP, omega-3 index, CAC score when indicated) and create a personalized plan to reduce total atherogenic burden — especially when the standard lipid panel is “normal,” but risk remains high.
🌀
Conclusion
Lp(a) is the main missed cardiology risk factor in an apparently healthy adult. One test. Once in a lifetime. A reference point for decades ahead.
For now, Lp(a) itself is almost impossible to lower substantially (RNA agents are expected in clinical practice from 2027). But we can aggressively control everything that depends on us: ApoB, BP, glycemia, inflammation, endothelium, and the omega-3 index. High Lp(a) is not a sentence; it is an instruction not to leave other factors in the red zone. When ApoB <65 mg/dL, BP <120/80, hsCRP <1, and omega-3 index >8%, Lp(a) no longer finds a vulnerable vessel.
Treat the vessel, not its complications.
🌀
Sources
▸Kronenberg F, Mora S, Stroes ESG, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. *Eur Heart J* 2022;43:3925–3946. PMID 36302098 ▸Tsimikas S. A test in context: lipoprotein(a). *J Am Coll Cardiol* 2017;69:692–711. PMID 28057251 ▸Clarke R, Peden JF, Hopewell JC, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. *N Engl J Med* 2009;361:2518–2528. PMID 20032323 ▸Mehta A, Virani SS, Ayers CR, et al. Lipoprotein(a) and family history predict cardiovascular disease risk. *J Am Heart Assoc* 2020;9:e014733. PMID 32063126 ▸Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, et al. Lipoprotein(a) reduction in persons with cardiovascular disease (AKCEA-APO(a)-LRx). *N Engl J Med* 2020;382:244–255. PMID 31893580
Related articles: Endothelium: foundation of vascular health, Cholesterol without statins.
🌀
FAQ
If Lp(a) is high, can it be lowered? On your own — almost no. Diet, exercise, and statins do not work. Apheresis (plasmapheresis) produces a 60–80% reduction per session, but the procedure is expensive and not available everywhere. PCSK9 inhibitors lower Lp(a) by 25–30%. RNA agents (pelacarsen, olpasiran) are in phase 3, with expected clinical entry in 2027.
Why test Lp(a) if I cannot do anything about it anyway? Because you can do a lot with the other factors. Lp(a) > 50 mg/dL shifts the targets: ApoB <65 (not <80), BP <120/80 (not <140/90), omega-3 index >8%, and discussion of aspirin. Without knowing Lp(a), you are aiming at the wrong target.
Does pregnancy affect Lp(a)? Yes. In the second half of pregnancy, Lp(a) physiologically increases by 50–100%. Therefore the initial test should be done outside pregnancy. If the result is elevated only during pregnancy, this is not a diagnosis but a physiologic rise.
At what age does it make sense to test Lp(a) in children? With a strong family history (early myocardial infarction in a parent, known Lp(a) > 50 mg/dL in a parent) — from age 5–10. In the general population — after age 18, but in any case, sooner or later it is worth doing for everyone.
What should be done if Lp(a) is very high (>180 mg/dL, >450 nmol/L)? Full cardiology screening: ApoB, advanced lipid panel, hsCRP, CAC score, carotid ultrasound. Aggressive ApoB control to <65 mg/dL (statin + ezetimibe ± PCSK9), BP <120/80, smoking cessation, omega-3 2–4 g/day. Screening of children and siblings. Discussion of aspirin and apheresis individually with a cardiologist.
*This article is for informational purposes and does not replace medical consultation. Before starting any nutraceuticals, changing medication therapy, or undergoing diagnostic procedures, discuss the plan with your treating physician.*
References
- PMID 36302098. PMID 36302098
- PMID 28057251. PMID 28057251
- Clarke R, Peden JF, Hopewell JC, et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med 2009;361:2518–2528. PMID 20032323
- Mehta A, Virani SS, Ayers CR, et al. Lipoprotein(a) and family history predict cardiovascular disease risk. J Am Heart Assoc 2020;9:e014733. PMID 32063126
- Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, et al. Lipoprotein(a) reduction in persons with cardiovascular disease (AKCEA-APO(a)-LRx). N Engl J Med 2020;382:244–255. PMID 31893580