Introduction: recalculating the global burden
JAMA · STAT, March 30, 2026: after recalculation of the Global Burden of Disease using a new model of subclinical lead exposure, lead rose to 8th place among causes of death from ischemic heart disease — previously 18th. According to the new estimate, this represents 1.5 million deaths per year, most of them cardiovascular.
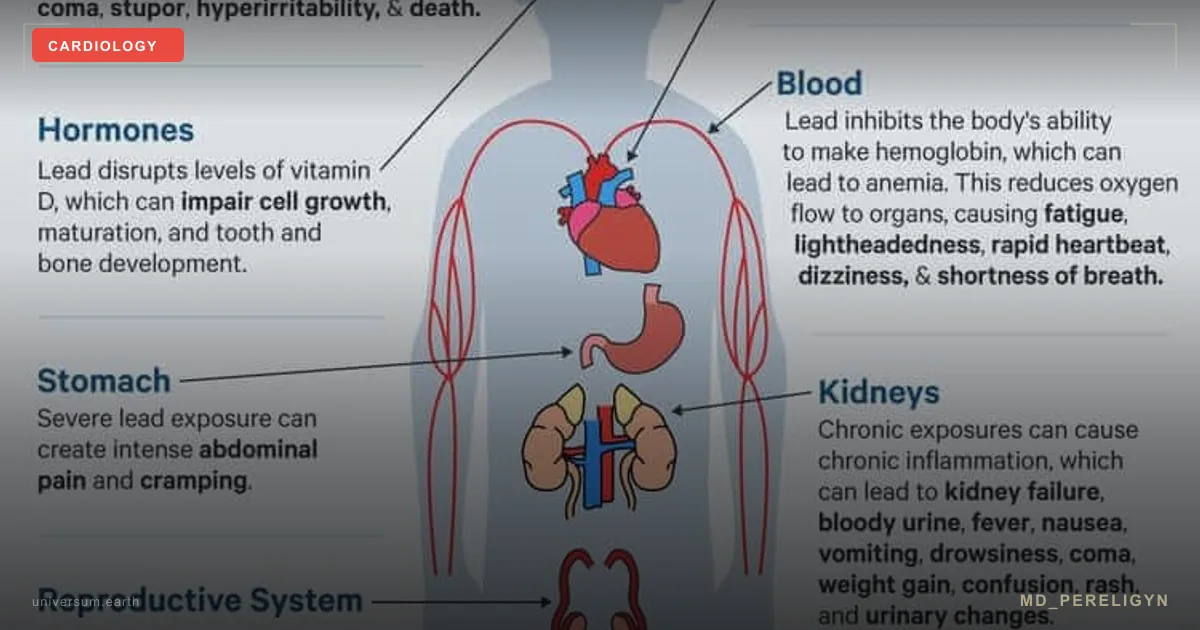
Lead is no longer a “pediatric” problem. It is a systemic cardiotoxin that damages the endothelium, raises blood pressure, accelerates atherosclerosis, and is associated with increased all-cause mortality even at concentrations below 5 μg/dL.
Core idea of the md_pereligyn protocol: lead is an invisible, asymptomatic cardiovascular risk factor. It does not show up on ECG, is not visible in a lipid panel, and is not diagnosed during a routine examination. Without targeted screening, it is missed for decades.
I work with this marker separately from the classic lipid panel — because without knowing blood lead concentration, it is impossible to assess the true myocardial infarction risk in a patient who grew up in an industrial city or renovated housing built before 1991.
🌀
Mechanism of cardiotoxicity
Lead damages the vascular system through several parallel mechanisms, and these mechanisms overlap with endothelial dysfunction described in the article on the endothelium.
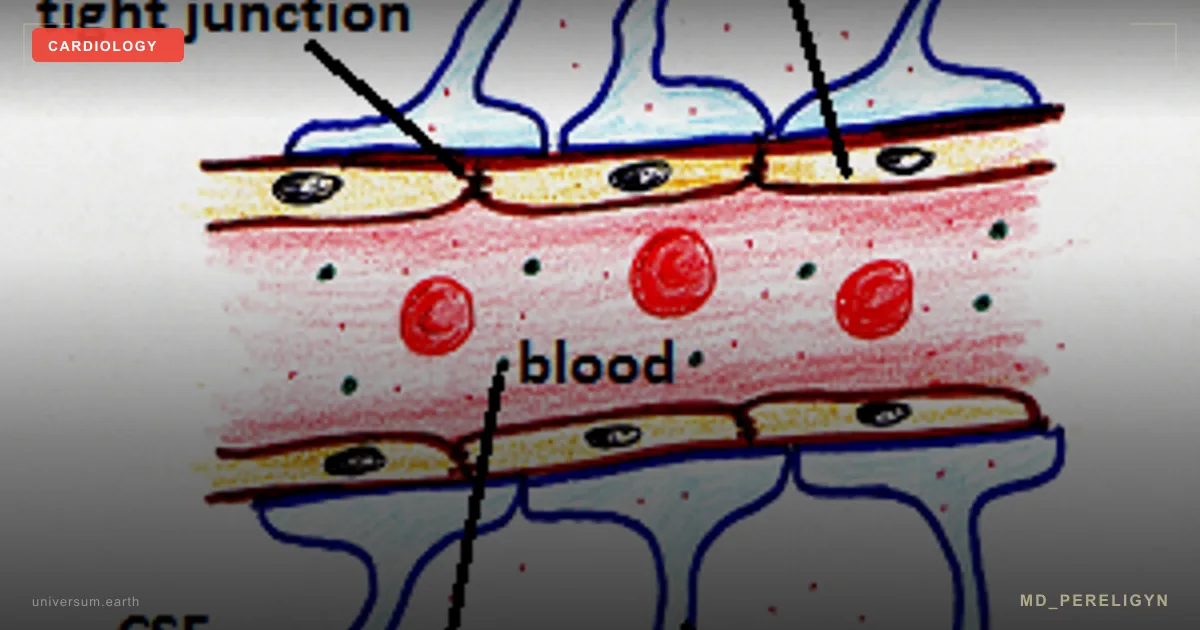
▸Blockade of eNOS and reduced NO. Pb²⁺ competes with Ca²⁺ for activating sites on endothelial NO synthase and disrupts eNOS phosphorylation. Nitric oxide bioavailability falls, and the endothelium loses its ability to relax. Arterial stiffness increases and blood pressure rises (Vaziri ND, Am J Physiol Heart Circ Physiol 2008, PMID 18599595[1]). ▸Oxidative stress. Pb stimulates NADPH oxidase and increases superoxide production. Superoxide destroys NO with formation of peroxynitrite, which damages proteins, DNA, and lipids. ▸LDL oxidation. Oxidized LDL penetrates through the damaged glycocalyx, is taken up by macrophages, and forms foam cells — the core of a future atherosclerotic plaque. ▸Increased blood pressure. Each doubling of blood lead concentration is associated with a 1.2–1.5 mmHg increase in systolic blood pressure and an approximately 30% higher risk of hypertension (Navas-Acien A, Environ Health Perspect 2007, PMID 17431500[2]). ▸Accelerated atherosclerosis and calcification. Pb displaces Ca²⁺ from the bone matrix, disrupts mineralization, and redirects calcium into the arterial wall. ▸Direct cardiotoxicity. Chronic exposure is linked to diastolic dysfunction, QT prolongation, and an increased risk of fatal arrhythmias.
Over decades, the process becomes clinically apparent: hypertension at 35, myocardial infarction at 50, stroke at 60. But the first steps — reduced FMD and increased ADMA — can be detected 15–20 years earlier.
🌀
Bone depot: the body’s 20–30-year memory
95% of lead in the body is stored in the bone matrix, where it replaces calcium in hydroxyapatite. The half-life in bone is 20–30 years. This means that exposure from the late 1980s — lead paint, leaded gasoline, soldered water risers — continues to act in 2026.
During periods of increased bone remodeling — pregnancy, lactation, menopause, osteoporosis, prolonged immobilization, keto diets with bone-mass loss — lead is mobilized back into the bloodstream. Plasma concentration rises without new exposure.
Therefore, a single BLL (blood lead level) measurement is insufficient to assess total body burden. Either K-XRF is needed (bone X-ray fluorescence, mainly a research tool), or an integrated assessment through hair analysis.
🌀
Drivers — sources of exposure
Six major sources relevant for the post-Soviet region and beyond:
•Paints before 1991. Lead pigments were not banned in the USSR before its collapse. Old layers on walls, doors, and windows in Khrushchev- and Brezhnev-era apartments. Sanding without a HEPA filter raises Pb dust, which settles in the airways and on the floor. •Soldered risers and brass taps. Lead-tin solder was used in plumbing until the 2000s. Pb leaches overnight when water is stagnant. Flushing the tap for 30 seconds in the morning reduces the concentration. •Soil around metallurgical sites. Kryvyi Rih, Mariupol, Zaporizhzhia, Dnipro, Norilsk, Chelyabinsk — decades of emissions have accumulated lead in soil. Vegetables from household garden plots in these zones are a concentrated source. •Renovation dust without a HEPA filter. Dry sanding of old walls generates Pb aerosol that settles on furniture and toys for months. •Ruins and construction dust after 2022. Destroyed buildings, especially prewar and Soviet-era structures, contain lead coatings and roofing materials. Pb dust spreads for kilometers. •Leaded aviation gasoline and old vehicles. General aviation and some vintage cars continue to use leaded fuel.
Also: ceramic tableware with uncertified glaze (especially bright red and yellow), “surma” / “kohl” cosmetics, some Ayurvedic preparations, and predatory fish from polluted waters (lead and methylmercury).
🌀
There is no safe dose
CDC reference value 3.5 μg/dL is the level at which intervention is required in children. For adults, no threshold exists. Even below 5 μg/dL, increases have been documented in:
▸all-cause mortality by 25% (Lanphear BP, Lancet Public Health 2018, PMID 29544878[3]), ▸cardiovascular mortality by 70%, ▸ischemic heart disease mortality by 109%, ▸risk of arterial hypertension by 22% with each doubling of BLL.
These data come from NHANES, a representative cohort of the US population, and are supported by JAHA 2021 (burden of proof) and WHO 2024.
Therapeutic target of the md_pereligyn protocol: BLL < 2 μg/dL. This is the lower sensitivity limit of most commercial laboratories and a realistic target with proper nutritional support and source elimination.
🌀
Markers and diagnostics
What to order when chronic lead burden is suspected — especially in patients with resistant hypertension, early atherosclerosis, unexplained nephropathy, or residence in industrial regions:
▸BLL (blood lead level) — standard venous blood test. Target level <2 μg/dL. Method: atomic absorption spectrometry or ICP-MS. ▸ZPP (zinc protoporphyrin) — rises when ferrochelatase is inhibited by lead. An indirect marker of chronic exposure; it does not replace BLL. ▸Hair Mineral Analysis — integrated assessment of heavy metals over 2–3 months. European reference: Ortho-Analytic AG (Switzerland, orthoanalytic.ch). Useful for screening “who is at risk,” but does not replace BLL for acute assessment. ▸Provocation challenge test — 24-hour urine after administration of a chelator (DMSA, EDTA). Used in specialized toxicology centers. Not a first-line tool. ▸Ionized calcium, phosphorus, PTH, 25(OH)D — assessment of bone matrix status (depot). ▸Creatinine, cystatin C, microalbuminuria — Pb nephropathy appears long before changes in glomerular filtration rate. ▸FMD, hsCRP, omega-3 index — assessment of secondary endothelial injury. ▸Ambulatory blood pressure monitoring (ABPM) — Pb-induced hypertension is often resistant to one medication.
For patients from industrial-risk zones, I recommend targeted screening every 2–3 years; with renovation/construction exposure, annually.
🌀
Holistic protocol: elimination and support
Principle of the md_pereligyn protocol: in lead burden, aggressive chelation without source elimination is pointless — Pb is mobilized from bone and reloads the blood. The strategy is two-stage: first stop exposure, then provide nutritional and, when indicated, pharmacological support for elimination.
### 1. Source elimination
▸Water filter: reverse osmosis or a carbon block certified to NSF/ANSI 53 for lead. Flush the tap for 30 seconds in the morning before use. ▸Renovation according to the EPA RRP standard: HEPA vacuum, wet cleaning, isolation of the work area. No dry sanding of old surfaces. ▸Vegetables from household garden plots in industrial zones — soil testing. Switch to certified producers. ▸Ceramic tableware: only FDA/EU-certified. No bright artisanal glaze for food use. ▸Cosmetics and supplements: avoid Ayurvedic preparations and “kohl” cosmetics without independent heavy-metal testing.
### 2. Nutritional competitors of Pb
Lead competes with calcium, iron, zinc, and magnesium for intestinal absorption and binding to transport proteins. Adequate status of these minerals reduces Pb bioavailability from food by tens of percent.
▸Calcium 1000–1200 mg/day — primarily from food (dairy if tolerated, leafy greens, sardines with bones). In osteoporosis, supplements with vitamin K2. ▸Iron — target ferritin 60–100 ng/mL. Iron deficiency increases Pb absorption 2–3-fold. ▸Zinc 15–30 mg/day — competes with Pb for metallothionein binding. ▸Magnesium (glycinate / taurate) 400 mg — eNOS cofactor, direct vascular relaxant. ▸Vitamin C 500–1000 mg — reduces Pb absorption and regenerates BH4 (eNOS cofactor).
### 3. Antioxidant support
Lead generates oxidative stress — parallel antioxidant protection is required.
▸N-acetylcysteine (NAC) 600–1200 mg — glutathione precursor, with demonstrated nephroprotection in Pb exposure (Pande M, Toxicology 2001, PMID 11369130[4]). ▸Alpha-lipoic acid 300–600 mg — chelating antioxidant, recycles glutathione and vitamin C. ▸Glutathione (liposomal) 250–500 mg or its precursors (glycine 3 g + cysteine 500 mg). ▸Selenium 100–200 μg — cofactor of glutathione peroxidase.
### 4. Elimination support
▸Fiber 30–40 g/day (psyllium, oats, legumes) — binds biliary Pb and prevents enterohepatic recirculation. ▸Chlorella 3–5 g/day or modified citrus pectin — mild dietary binders. The evidence base is limited; they are used as support, not as a substitute for medical chelation. ▸Adequate hydration and regular bowel movements — basic drainage support.
### 5. Endothelial support
Pb has already damaged eNOS — in parallel with elimination, the vessel itself needs support. The full protocol is in the article on the endothelium. Brief minimum:
▸L-citrulline 3 g/day — bypasses eNOS inhibition and increases plasma arginine. ▸Pomegranate (extract) 250–500 mg — punicalagin restores FMD (Aviram M, Atherosclerosis 2008, PMID 17726507[5]). ▸Omega-3 (EPA+DHA) 2 g/day — omega-3 index >8%. ▸Vitamin D3 + K2 — correction of deficiency, protection from arterial calcification.
### 6. Pharmacological chelation (when indicated)
With BLL >25 μg/dL in adults or symptomatic neuropathy — DMSA (succimer) orally, in 19-day courses under toxicologist supervision. Intravenous EDTA is an inpatient protocol and requires monitoring of kidney function and mineral balance.
Self-directed chelation without assessment of the source, mineral status, and kidney function is prohibited — there is a high risk of redistributing Pb into the brain and worsening neurotoxicity.
🌀
What does NOT work (and why)
▸Isolated “detox teas” and “antioxidant” supplements without source elimination — Pb continues to enter the body, so the effect is zero. ▸Self-directed DMSA/EDTA chelation without a physician — risk of redistributing lead into the CNS, mineral imbalance, nephrotoxicity. ▸Sauna and sweating — sweat removes negligible amounts of Pb compared with renal and biliary excretion. Useful for general health, but not as an elimination strategy. ▸Megadose chlorella without regular bowel movements — Pb may be reabsorbed. A binder works only together with fiber and normal transit. ▸Calcium without vitamin D and K2 — calcium is not absorbed efficiently and may deposit in the arterial wall. ▸Iron deficiency during Pb exposure — accelerated Pb absorption from the GI tract. The paradox: “treating anemia” becomes a priority for lead control.
🌀
When to seek evaluation
▸Resistant hypertension before age 50 ▸Early atherosclerosis without typical risk factors (normal cholesterol, non-smoker, no diabetes) ▸Unexplained nephropathy or microalbuminuria ▸History of living in an industrial zone (Kryvyi Rih, Mariupol, Zaporizhzhia, Dnipro, Norilsk, Chelyabinsk, similar regions) ▸DIY or occupational renovation of housing built before 1991 ▸Pregnancy, pregnancy planning, or lactation in the presence of any of the factors above ▸Nonspecific cognitive complaints (brain fog, reduced concentration) in patients from risk groups
I perform complete toxicological screening (BLL, ZPP, hair mineral analysis), assess vascular and renal status, and build a personalized two-stage protocol: source elimination + nutritional support +, when indicated, pharmacological chelation under toxicologist supervision.
🌀
Conclusion
Lead is a hidden cardiotoxin that damages the endothelium, raises blood pressure, accelerates atherosclerosis, and is associated with increased mortality even at concentrations below 5 μg/dL. There is no safe dose. The bone depot preserves decades of exposure and continues to act today.
The strategy is two-stage: eliminate the source (water, renovation, soil, tableware, cosmetics) → nutritional support (Ca, Fe, Zn, Mg, NAC, ALA, fiber, endothelial protocol). At high BLL — pharmacological chelation under toxicologist supervision.
Without targeted screening, lead burden is missed for decades. In patients from industrial regions and those who have worked on renovating old housing, BLL measurement should become routine — at least once every 2–3 years.
🌀
Sources
▸Lanphear BP, Rauch S, Auinger P, et al. Low-level lead exposure and mortality in US adults. *Lancet Public Health* 2018;3:e177–e184. PMID 29544878 ▸Navas-Acien A, Guallar E, Silbergeld EK, Rothenberg SJ. Lead exposure and cardiovascular disease — a systematic review. *Environ Health Perspect* 2007;115:472–482. PMID 17431500 ▸Vaziri ND. Mechanisms of lead-induced hypertension and cardiovascular disease. *Am J Physiol Heart Circ Physiol* 2008;295:H454–H465. PMID 18599595 ▸Pande M, Mehta A, Pant BP, Flora SJ. Combined administration of NAC and meso-2,3-dimercaptosuccinic acid reduces lead-induced oxidative stress. *Toxicology* 2001;162:127–137. PMID 11369130 ▸Aviram M, Rosenblat M. Pomegranate juice and atherosclerosis. *Atherosclerosis* 2008;200:39–45. PMID 17726507 ▸GBD 2026 Risk Factors Collaborators. Global burden update — lead exposure ranks 8th for ischemic heart disease mortality. *JAMA* 2026 (STAT report, 30.03.2026). ▸WHO 2024. Childhood lead poisoning prevention: blood lead reference value 3.5 μg/dL. ▸Bahadoran Z, Mirmiran P, Ghasemi A. Role of nitric oxide in vascular health. *Nutr Metab (Lond)* 2021;18:23. PMID 34167581
Related articles: Endothelium: the foundation of vascular health, Cholesterol without statins.
🌀
FAQ
If I live in a large city, should I worry about lead? In modern cities, the main source is old housing (paint, soldered risers) and renovation dust, not air. Leaded automotive gasoline has been banned since the 2000s. If the apartment was built before 1991 and has not undergone major renovation, it is reasonable to test BLL and check water for Pb. Especially during pregnancy, pregnancy planning, and renovation work.
Is it safe to chelate lead with self-purchased DMSA or EDTA? No. Uncontrolled chelation mobilizes Pb from bone and may redistribute it into the brain and kidneys. It also disrupts zinc, copper, and iron balance. Chelation is an inpatient or outpatient protocol under toxicologist supervision with monitoring of minerals and kidney function.
Which is more important — hair analysis or blood testing? For acute and recent exposure — BLL (blood lead level). For an integrated assessment over 2–3 months — hair mineral analysis. Ideally, do both. Hair analysis is useful for screening “who is at risk” within a family; BLL is required to decide on chelation.
Does sauna help eliminate lead? Sweat removes negligible amounts of Pb compared with urine and bile. Sauna is useful for general vascular health and stress resilience, but not as a heavy-metal elimination strategy. Do not rely on “detox through sweat.”
What should a pregnant woman with confirmed Pb burden do? Chelation during pregnancy is contraindicated (toxic for the fetus and mobilizes Pb from bone into the maternal bloodstream). Strategy: source elimination + strict nutritional support (calcium, iron, zinc, vitamin C, omega-3). After lactation — reassessment and decision about chelation.
*This article is for informational purposes and does not replace medical consultation. Before starting any nutraceuticals, changing medication therapy, or undergoing diagnostic procedures, discuss the plan with your treating physician.*
References
- PMID 18599595. PMID 18599595
- PMID 17431500. PMID 17431500
- PMID 29544878. PMID 29544878
- PMID 11369130. PMID 11369130
- PMID 17726507. PMID 17726507
- Bahadoran Z, Mirmiran P, Ghasemi A. Role of nitric oxide in vascular health. Nutr Metab (Lond) 2021;18:23. PMID 34167581