Introduction: hypertension is not about salt
In public communication, blood pressure (BP) is reduced to a single regulator: table salt. This is convenient for advertising low-salt products, but physiologically inaccurate. In practice, sodium is not the main driver in one third of patients with resistant hypertension (Calhoun DA, J Am Coll Cardiol 2008, PMID 19057981[1]).
Systematic reviews of randomized controlled trials (RCTs) show that the effect of a low-salt diet on systolic BP is 4–5 mm Hg on average. This is useful, but modest (Ettehad D, Lancet 2016, PMID 26724178[2]). By contrast, sleep apnea or chronic stress can produce an increase of +20 mm Hg or more.
Key idea of the md_pereligyn protocol: if blood pressure remains high on a salt-free diet, salt is not the problem. Six hidden drivers more often remain outside the field of view of standard outpatient care.
Hypertension is a symptom. Unsuccessful attempts to “remove salt” while ignoring the other regulators are a ritual, not treatment.
🌀
Physiology of BP regulation
Blood pressure is maintained by three circuits:
▸Sympathetic nervous system — immediate regulation through α- and β-adrenoceptors: arteriolar constriction, increased heart rate, and increased contractility. ▸RAAS (renin-angiotensin-aldosterone system) — intermediate-term regulation through angiotensin II (vasoconstrictor), aldosterone (sodium and water retention), and ADH. ▸Endothelium and vascular wall — local regulation through NO (vasodilation), endothelin-1 (vasoconstriction), prostacyclin, and vascular stiffness.
Salt acts on only one of the three circuits: RAAS, through volume load. If the other two are overloaded, diet will give 4 mm Hg and no more.
In younger patients, sympathetic tone predominates. In patients with metabolic syndrome, RAAS and endothelin predominate. In older adults, arterial stiffness predominates. There is no universal target.
🌀
Six hidden drivers
Each of the six factors can independently raise BP by 5–25 mm Hg. In combination, the effect is multiplicative.
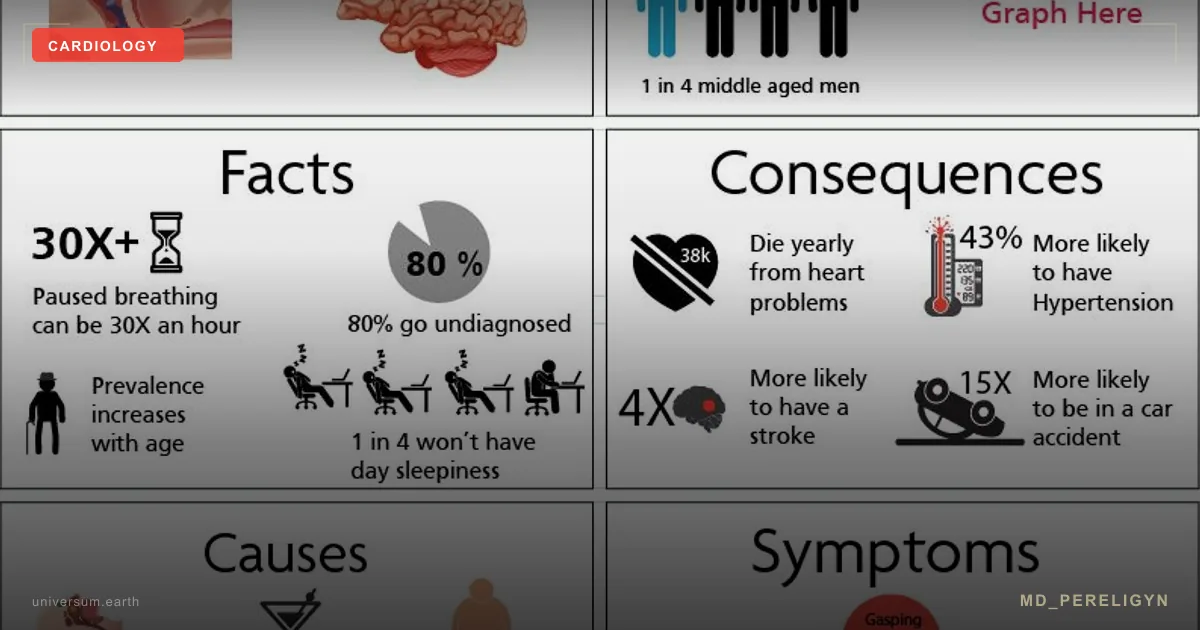
•Chronic stress — sustained activation of the sympathetic nervous system, increased cortisol, vasoconstriction, tachycardia, and arteriolar remodeling. Systolic BP rises by 5–15 mm Hg over several months of chronic stress. •Sleep apnea — intermittent hypoxia → nocturnal RAAS activation → nighttime BP peaks and morning hypertension. In 30–50% of patients with resistant hypertension, obstructive sleep apnea remains undiagnosed. •Visceral fat — adipokines (leptin, RBP4 — retinol binding protein 4) and insulin resistance are independent predictors of BP even with normal BMI. Each centimeter of waist circumference adds ~1 mm Hg. •Chronic inflammation — hsCRP (high-sensitivity C-reactive protein) >2 mg/L is an independent factor in vascular stiffness and endothelial dysfunction (Ridker PM, NEJM 2008, PMID 18997196[3]). •Magnesium deficiency — Mg²⁺ modulates arteriolar tone by blocking calcium channels and activating eNOS. Deficiency is a common but rarely checked source of “essential” hypertension. •Sleep deficiency and fructose — <6 hours of sleep over a week causes sustained sympathetic activation and an evening BP increase. Fructose >50 g/day (sweetened beverages, high-fructose syrup) increases uric acid and activates RAAS.
The seventh factor, arterial stiffness, is discussed in the endothelium article.
🌀
Markers and diagnostics
The standard approach of “measured in the office, prescribed a drug” misses 4 of the 6 drivers. What actually shows the picture:
▸24-hour ambulatory blood pressure monitoring (ABPM) — the gold standard. Detects nocturnal hypertension (typical of apnea), morning surge, white-coat hypertension, and masked hypertension. Target nocturnal dipping >10%. ▸Polysomnography or apnea screening (STOP-BANG questionnaire, home test) in the presence of snoring, morning hypertension, or daytime sleepiness. ▸hsCRP — target <1 mg/L. >3 mg/L indicates high vascular risk. ▸Fasting insulin, HOMA-IR — index of insulin resistance (homeostasis model assessment of insulin resistance). Target HOMA-IR <2.0. ▸HbA1c, fasting glucose — prediabetes with HbA1c 5.7–6.4% already increases BP and vascular risk. ▸Erythrocyte Mg²⁺ — not plasma magnesium (plasma is less informative and does not reflect the intracellular pool). ▸Aldosterone / renin (ARR) — to exclude primary hyperaldosteronism (5–10% of all hypertension cases). ▸TSH, morning cortisol — hyperthyroidism and hypercortisolism are common secondary causes. ▸Sleep tracker for one week + stress diary — subjective, but valuable for identifying patterns.
Target BP ranges (ESC 2024, ACC/AHA 2017): daytime office <130/80, home <125/75, nocturnal mean <115/65.
🌀
Holistic protocol
The principle of the md_pereligyn protocol: treatment targets the cause, not the number. Medications produce a rapid effect, but they do not eliminate the drivers. A holistic protocol restores regulation.
### 1. Reducing sympathetic tone
▸Breathing practices 10–20 min/day — slow diaphragmatic breathing (6 cycles/min) lowers systolic BP by 4–8 mm Hg over 8 weeks. ▸HRV training (heart rate variability) through biofeedback or apps. ▸Magnesium (glycinate / taurate) 400 mg — a cofactor of parasympathetic regulation and a direct vascular relaxant. ▸Yoga, tai chi 3 times/week — lower BP comparably to low-dose monotherapy.
### 2. Treating apnea
▸Weight loss when BMI >27 — 5–10% body weight loss significantly improves AHI (apnea-hypopnea index). ▸Positional therapy — avoiding supine sleep in patients with positional apnea. ▸CPAP when AHI >15 — the gold standard; lowers nocturnal BP by 5–10 mm Hg. ▸Mandibular advancement device (MAD) for mild to moderate disease. ▸Avoid alcohol for 4 hours before sleep — alcohol worsens obstructive episodes.
### 3. Reducing visceral fat
▸Mediterranean / DASH pattern — olive oil, fish, vegetables, nuts, legumes. Reduction in systolic BP by 8–14 mm Hg. ▸Restriction of fast carbohydrates and fructose — fructose >50 g/day activates RAAS and increases uric acid. ▸Strength training 2–3 times/week — support for muscle mass and insulin sensitivity. ▸Intermittent fasting 14:10 / 16:8 — improved HOMA-IR and reduced visceral fat depot.
### 4. Magnesium and minerals
▸Magnesium (glycinate / taurate) 400 mg/day — reduction in systolic BP by 2–4 mm Hg in a meta-analysis of RCTs. ▸Potassium 4–5 g/day from diet — leafy greens, avocado, legumes, potatoes with skin. Each 1000 mg of potassium lowers systolic BP by 2–3 mm Hg. ▸Na/K ratio is more important than absolute sodium. Target <1.0. ▸Calcium — 1000 mg/day from diet (dairy, leafy greens).
### 5. Anti-inflammatory pool
▸Omega-3 EPA+DHA 2 g/day — BP reduction by 2–4 mm Hg, anti-inflammatory effect. ▸Curcumin 500–1000 mg with piperine — reduction in hsCRP, endothelial protection. ▸Polyphenols — cocoa (flavanols 500 mg), pomegranate (250–500 mg extract), extra virgin olive oil. ▸Restriction of omega-6 / trans fats — sunflower and corn oil, fast food.
### 6. Sleep and stress
▸Sleep 7–9 hours in a stable window — the main regulator of sympathetic tone. ▸Morning light 10–20 min — circadian rhythm synchronization, lower evening cortisol. ▸Alcohol restriction — each 10 g of ethanol raises systolic BP by 1 mm Hg. ▸Caffeine <300 mg/day and no later than 14:00. ▸Cold exposure or sauna 2–4 times/week — vagal tone and endothelial adaptation.
### 7. Vitamin D + K2
▸Vitamin D3 to a level of 50–80 ng/mL, with individualized doses of 2,000–5,000 IU/day. ▸Vitamin K2 (MK-7) 100–200 mcg — directs calcium into bone and protects against arterial calcification.
### 8. Pharmacotherapy: when it is needed
A holistic protocol does not replace medication in severe or symptomatic hypertension. With BP >160/100, target-organ damage, or high 10-year risk, medications are used together with the protocol, not instead of it.
First-line drugs (ESC 2024): ACE inhibitors or ARBs + calcium channel blockers or thiazide diuretics. The decision is individualized with the treating physician.
🌀
What does NOT work
▸Isolated “remove salt” while ignoring the 5 other drivers — gives 4 mm Hg and no more. ▸Short-term “one-week” diets — BP returns without sustained pattern change. ▸Cardiomagnetic bracelets, “blood pressure” supplements without an evidence base — loss of time and money. ▸Stopping medication without physician supervision — abrupt withdrawal of beta-blockers causes a rebound effect and myocardial infarction risk. ▸Ignoring apnea in the presence of snoring and morning hypertension — the main missed driver. ▸High doses of caffeine and energy drinks — an acute increase of 5–10 mm Hg and chronic sympathetic activation.
🌀
When to seek care
▸BP >140/90 on three measurements on different days ▸BP >130/80 combined with diabetes, CKD, or metabolic syndrome ▸Morning hypertension, nocturnal dipping <10% ▸Snoring, daytime sleepiness, Epworth score >10 ▸Resistant hypertension (BP remains high on 3 medications) ▸Family history of early strokes / myocardial infarctions before age 60 ▸hsCRP >2 mg/L on repeat testing
I perform a complete screening assessment (ABPM, apnea screening, hormonal profile, extended biochemistry, endothelial markers) and develop a personalized protocol that accounts for all six drivers.
🌀
Conclusion
Hypertension is a symptom, not a diagnosis. Behind the number 145/95 is a specific set of drivers: sympathetic tone, RAAS, apnea, insulin resistance, magnesium deficiency, and inflammation. In one patient, one circuit dominates; in another, three do.
A holistic protocol — reducing sympathetic tone, treating apnea, addressing visceral fat, restoring the mineral pool, anti-inflammatory nutraceuticals, sleep, and movement — lowers systolic BP by 10–25 mm Hg over 3–6 months. Medications remain necessary in severe disease, but in combination with the protocol, not instead of it.
Regulation should be treated, not the number.
🌀
Sources
▸SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. *NEJM* 2015;373:2103–2116. PMID 26551272 ▸Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death. *Lancet* 2016;387:957–967. PMID 26724178 ▸Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. *J Am Coll Cardiol* 2008;51:1403–1419. PMID 19057981 ▸Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated CRP. *NEJM* 2008;359:2195–2207. PMID 18997196 ▸Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA hypertension guideline. *J Am Coll Cardiol* 2018;71:e127–e248. PMID 29133356 ▸Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension. *J Hypertens* 2023;41:1874–2071. PMID 37345492
Related articles: Endothelium: foundation of vascular health, Cholesterol without statins.
🌀
FAQ
Can blood pressure medications be stopped if lifestyle is addressed? Sometimes yes, but only under physician supervision and gradually. In mild hypertension (140–150/90) with a sustained protocol effect (BP <130/80 for 3–6 months), medications can be reduced or stopped. In severe disease, target-organ damage, or high 10-year risk, medications remain necessary. Abrupt self-discontinuation is unacceptable.
What minimum tests should be done first? Home BP monitoring for 7 days in the morning and evening, 24-hour ABPM, apnea screening (STOP-BANG), hsCRP, HbA1c, fasting insulin, creatinine, urinalysis with microalbuminuria, electrolytes, TSH. If indicated: ARR, cortisol, metanephrines. Full screening and interpretation are performed during consultation.
Does the DASH diet help without other interventions? Yes, but the effect is limited. DASH lowers systolic BP by 8–11 mm Hg when followed strictly. This is good, but insufficient when combined with apnea or high insulin resistance. Diet is the foundation, not monotherapy.
How soon should BP reduction be expected on the protocol? The effect of magnesium and potassium appears after 2–4 weeks. The effect of CPAP begins on the first night. The effect of DASH and weight loss appears after 4–8 weeks. The effect of the full protocol is a sustained reduction of 10–25 mm Hg over 3–6 months. ABPM should be repeated every 3 months.
Should blood pressure be measured every day? Yes. During the first 3 months of the protocol: in the morning (before medications and coffee) and in the evening, with 2 measurements 1 minute apart. The weekly average is the working number. After stabilization: once per week. Excessively frequent measurements provoke anxiety and distort the picture.
*This article is for informational purposes only and is not a substitute for professional medical advice. Discuss any nutraceutical, medication adjustment, or diagnostic procedure with your treating physician before starting.*
References
- PMID 19057981. PMID 19057981
- PMID 26724178. PMID 26724178
- PMID 18997196. PMID 18997196
- SPRINT Research Group. A randomized trial of intensive versus standard blood-pressure control. NEJM 2015;373:2103–2116. PMID 26551272
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA hypertension guideline. J Am Coll Cardiol 2018;71:e127–e248. PMID 29133356
- Mancia G, Kreutz R, Brunström M, et al. 2023 ESH Guidelines for the management of arterial hypertension. J Hypertens 2023;41:1874–2071. PMID 37345492